Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- According to U.S. Surgeon General Dr. Vivek Murthy, if you’ve already recovered from a bout of COVID-19, the immunity mounted by your body may not be enough to prevent reinfection with the Delta variant, so your best bet is to get the COVID shot
- August 6, 2021, the U.S. Centers for Disease Control and Prevention published a case control study claiming that unvaccinated people are “more than twice as likely to be reinfected with COVID-19 than those who were fully vaccinated after initially contracting the virus”
- One of several drawbacks of this study is that it did not look at illness severity. It doesn’t tell us whether more vaccinated people were symptomatic than the unvaccinated, or vice versa
- A far better gauge of how well the COVID jabs are working would be serious infection, hospitalization and death rates, and when we look at those, a different picture emerges
- In Israel — where data suggest those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection — a majority of serious cases and deaths are occurring among those injected with two doses of Pfizer’s mRNA jab
According to U.S. Surgeon General Dr. Vivek Murthy, if you’ve already recovered from a bout of COVID-19, the full-spectrum immunity mounted by your body may not be enough to prevent reinfection with the Delta variant, so your best bet is to get the COVID shot. Mid-August 2021 he told CNN:1
“… what we’ve understood, actually, from the studies about natural immunity, we are seeing more and more data that tells us that while you get some protection from natural infection, it’s not nearly as strong as what you get from the vaccine, especially with the Delta variant, which is the hardiest and most contagious variant we’ve seen to date. We need all the protection that we can get. That’s why the vaccines are so effective.”
Data Analysis Claims Unvaccinated More Prone to Reinfection
August 6, 2021, the U.S. Centers for Disease Control and Prevention published a case control study2,3 claiming that unvaccinated people are “more than twice as likely to be reinfected with COVID-19 than those who were fully vaccinated after initially contracting the virus.”
The study used data reported to Kentucky’s National Electronic Disease Surveillance System (NEDSS) to assess SARS-CoV-2 reinfection rates in Kentucky during May through June 2021 among those who’d had confirmed SARS-CoV-2 infection between March and December 2020.
The NEDSS data were then imported into a REDCap database that tracks new COVID-19 cases. A case-patient was defined as a resident with laboratory-confirmed SARS-CoV-2 infection in 2020 and a subsequent positive test result during May 1, 2021, through June 30, 2021.
Vaccination status was determined using data from the Kentucky Immunization Registry. Patients were considered fully vaccinated if a single dose of Johnson & Johnson or a second dose of an mRNA vaccine (Pfizer or Moderna) had been administered at least 14 days before reinfection. Compared to fully vaccinated residents, unvaccinated residents were 2.34 times more likely to test positive for SARS-CoV-2 reinfection.
The Obvious Flaw in CDC’s Study
The elephant in the room, however, is the absence of actual symptomatic illness. The study only looked at positive test results, and we do not know whether more vaccinated people were symptomatic than the unvaccinated, or vice versa.
As has been explained many times before, a positive test result is not the same as active infection. A person with natural immunity may be re-exposed to the virus, and traces of it may show upon testing, but their immune system has effectively killed the virus and prevented illness.
So, merely looking at positive test results is not the best way to ascertain whether the COVID jab actually provides better protection than natural immunity. And there are many reasons to suspect that it does not.
Other Shortcomings
The study authors also admit there are several other limitations to the findings, including the following:4
“First, reinfection was not confirmed through whole genome sequencing, which would be necessary to definitively prove that the reinfection was caused from a distinct virus relative to the first infection …
Second, persons who have been vaccinated are possibly less likely to get tested. Therefore, the association of reinfection and lack of vaccination might be overestimated. Third, vaccine doses administered at federal or out-of-state sites are not typically entered in KYIR, so vaccination data are possibly missing for some persons in these analyses …
Fourth, although case-patients and controls were matched based on age, sex, and date of initial infection, other unknown confounders might be present. Finally, this is a retrospective study design using data from a single state during a 2-month period; therefore, these findings cannot be used to infer causation.”
It is correct that association does not equate to causation, and we’ve been repeatedly told to dismiss Vaccine Adverse Event Reporting System (VAERS) data for this very reason. Perhaps the same standard should be applied to this CDC investigation, as it tells us very little about the actual risk associated with reinfection.
For all we know, those with natural immunity tested positive for reinfection but had no symptoms, while vaccinated people tested positive and were actually ill. Which, in that case, would be the preferable outcome?
Hospitalization and Mortality Rates Are a Better Gauge
A far better gauge of how well the COVID jabs are working would be serious infection, hospitalization and death rates, and when we look at those, a different picture emerges.
In Israel, where vaccine uptake has been very high due to restrictions on freedom for those who don’t comply,5 data show those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection.6,7,8
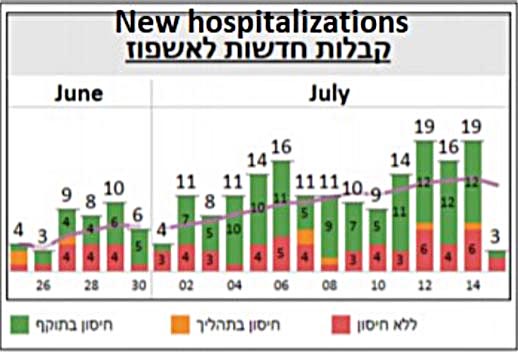
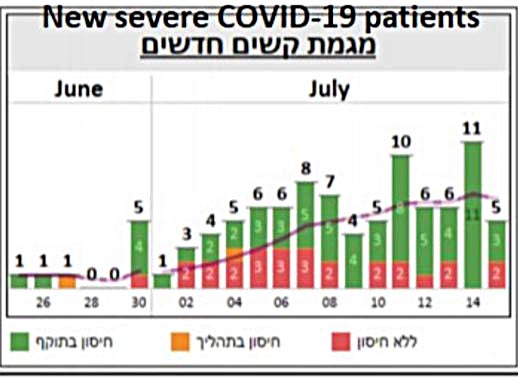
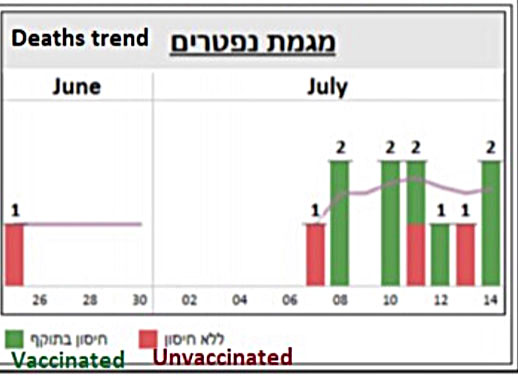
That too refers to test results, so let’s look at hospitalization rates instead. Here, we find a majority of serious cases and deaths are in fact occurring among those injected with two doses.
The following is a screenshot of graphs posted on Twitter.9 The red is unvaccinated, yellow refers to partially “vaccinated” and green fully “vaccinated” with two doses. The charts speak for themselves.
Do not be deceived by claims that unvaccinated patients make up 99% of COVID-19 deaths and 95% of COVID-related hospitalizations in the United States.10
These statistics were manufactured by looking at hospitalization and mortality data from January through June 2021 — a time frame when COVID jab rates were low. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot so, clearly, unvaccinated made up the bulk of COVID-related hospitalizations last winter. By mid-April, an estimated 31% had received one or more shots,11 and as of June 30, just 46.9% were “fully vaccinated.”12
Why COVID Shot Cannot End COVID Outbreaks
Overall, it doesn’t appear as though COVID-19 gene modification injections have the ability to effectively eliminate COVID-19 outbreaks, and this makes sense, seeing how it’s mathematically impossible for them to do so.
The four available COVID shots in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.13,14 (Efficacy rates of 67% to 95% all refer to the relative risk reduction.) Meanwhile, the noninstitutionalized infection fatality ratio across age groups is a mere 0.26%.15
Since the absolute risk that needs to be overcome is lower than the absolute risk reduction these injections can provide, mass vaccination simply cannot have a favorable impact, even with a vaccination rate of 100%.
Don’t believe it? There’s proof. July 14, 2021, BBC News reported16 there’d been an outbreak on the British Defense aircraft carrier HMS Queen Elizabeth. Despite the entire crew being fully injected, 100 crew members tested positive. (It’s unclear whether any of them actually had symptoms.)
The recent outbreak onboard a Carnival cruise line ship is another example. All crew and passengers had presented proof of being jabbed, yet that didn’t prevent an outbreak from taking place.17
The reason is very simple. Just as we have been telling you from the beginning, the shot does not prevent you from getting infected with the virus or spreading it around. “Vaccinated” individuals have actually been shown to be just as infectious as unvaccinated people. Even if they have fewer or milder symptoms, their viral load is just as great when infected, according to the CDC.18
There’s No Control Group to Compare Against Anymore
For some reason, government leaders and health officials want a needle in every arm, and they don’t care what the side effects of the shots might be. This is evident by the fact that we now have tens of thousands of reported deaths (according to one whistleblower, 45,000 deaths have occurred within three days of injection19,20) and well over half a million injury reports following COVID “vaccination,”21 yet no action is taken to slow down or halt the campaign.
Historically, mass vaccination campaigns have been halted and drugs withdrawn after 25 to 50 deaths (depending on the product). We’re so far past that now, one wonders if there actually is a threshold at which authorities will take action to protect the public from unnecessary medical injury and death.
VAERS is tricky to maneuver, so the easiest way to get a glimpse into the current status is to go to OpenVAERS.com, where you get a simple summary breakdown of current COVID-related reports.
Equally telling is the fact that all control groups have been eliminated from the still-ongoing injection trials,22 with full support from a World Health Organization Expert Working Group23 so, in the end, we’ll have no way of really evaluating side effects.
This is the perfect way to hide the truth about these shots, and it violates the very basics of what a safety trial has always been required to have. You simply must incorporate a control group to compare the effects of the drug against in the long term, otherwise you will have no clue as to what complications have arisen.
Safety evaluations have also been intentionally undermined by the U.S. Food and Drug Administration, which chose not to require vaccine makers to implement robust post-injection data collection and follow-up on the general public.
On top of that, the trials also do not appear to have oversight boards, which is standard practice for all human clinical trials. There’s no Data Safety Monitoring Board, no Clinical Event Committee and no Clinical Ethics Committee. How could this be?
If vaccine makers simply forgot to follow standard practices, it would mean we’re dealing with a truly staggering level of incompetence, as all COVID jab developers have made the same mistake. Which might be worse in this case? Intentional negligence or unintentional incompetence?
COVID-19 Shots Confer Narrow Immunity
Getting back to the issue of whether the COVID jab actually confers better protection against SARS-CoV-2 and its variants, this is highly unlikely seeing how the shot confers a very narrow and specific kind of protection, whereas natural immunity is broad.
When it comes to SARS-CoV-2 — which is clearly a genetically manipulated virus designed to attack your cardiovascular system and basic immune function — the spike protein is the most dangerous part and acts as a toxin in and of itself. This is why the spike protein was chosen as the antigen in these shots, but it’s also why so many are having side effects from them.
When you get a COVID shot, your body is instructed to manufacture the spike protein. In response, your body then produces antibodies against that spike protein. Those antibodies recognize only the spike protein and not other parts of the virus.
When you recover from a natural infection, your body has antibodies against all parts of the virus, so the spike protein plus four other proteins. In addition to that, you have memory T cells, which appear even more important than antibodies when it comes to battling viruses.
Does it make sense that one type of antibody would be more effective against a virus that may have mutated one or more of its proteins? Or is it more likely that having several types of antibodies plus memory T cells will offer greater protection?
If you pay attention, you will find that no one ever offers a sensible explanation as to why a single anti-spike antibody would be better than T cells and antibodies against all parts of the virus.
Natural Immunity Is Robust and Long-Lasting
Many studies have been published demonstrating that natural immunity against SARS-CoV-2 is both robust and long-lasting. For example, a May 2020 study24,25 found 70% of samples from patients who had recovered from mild cases of COVID-19 had resistance to SARS-CoV-2 on the T-cell level.
Interestingly, 40% to 60% of people who had not been exposed to SARS-CoV-2 also had resistance to the virus on the T-cell level. According to the authors, this suggests there’s “cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.”
A German paper26 came to a similar conclusion. Here, they found helper T cells that targeted the SARS-CoV-2 spike protein in 15 of 18 patients hospitalized with COVID-19. Yet another study,27,28,29 this one by Singaporean researchers, found common colds caused by the betacoronaviruses OC43 and HKU1 might make you more resistant to SARS-CoV-2 infection.
What’s more, they found that patients who became infected with the original SARS virus back in 2003 still had memory T cell immunity against SARS-CoV-2, despite the virus being only 80% similar. This study suggests natural immunity is likely to last decades, not months, like the COVID shot.
Unvaccinated Falsely Accused of Being ‘Disease Factories’
While mainstream media are now pushing the idea that those who refuse the COVID shot are to blame for the emergence of SARS-CoV-2 variants, a number of health experts have warned that the complete opposite scenario would occur — that mass injections, causing a very narrow band of antibodies, will force more rapid mutations of the virus.30
A general principle in biology, vaccinology and microbiology is that if you put living organisms like bacteria or viruses under pressure, via antibiotics or antibodies, for example, but don’t kill them off completely, you can inadvertently encourage their mutation into more virulent strains. Those that escape your immune system end up surviving and selecting mutations to ensure their further survival.
If an individual who does not have a narrow band of antibodies becomes infected, then, if mutation does occur, it’s far less likely to result in a more aggressive virus. So, while mutation can occur in both vaccinated and unvaccinated people, vaccinated individuals are actually far more likely to pressure the virus into a mutation that strengthens it and makes it more dangerous.
CDC Misrepresents Data to Push Jab on Those With Immunity
So far, the CDC has refused to change its stance on the matter. Instead, officials at the agency seem to have doubled down and actually go out of their way to misrepresent data in an effort to harass those with natural immunity to inappropriately take the jab, which is clinically unnecessary and potentially dangerous.
In a report issued by the CDC’s Advisory Committee on Immunization Practices (ACIP) December 18, 2020, the Pfizer-BioNTech COVID-19 vaccine was said to have “consistent high efficacy” of 92% or more among persons with underlying medical conditions as well as among participants with evidence of previous SARS-CoV-2 infection.31
After looking at the Pfizer trial data, Rep. Thomas Massie — a Republican Congressman for Kentucky and an award-winning scientist — discovered that’s completely wrong. In a January 30, 2021, Full Measure report, investigative journalist Sharyl Attkisson described how Massie tried, in vain, to get the CDC to correct its error. According to Massie:32,33
“There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either … It [the CDC report] says the exact opposite of what the data says.”
After multiple phone calls, CDC deputy director Dr. Anne Schuchat finally acknowledged the error and told Massie it would be fixed. “As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it,” Schuchat said in the recorded call.
January 29, 2021, the CDC issued its supposed correction, but rather than fix the error, they simply rephrased the mistake in a different way. This was the “correction” they issued:
“Consistent high efficacy (?92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
As you can see, the “correction” still misleadingly suggests that vaccination is effective for those previously infected, even though the data showed no such thing.
I don’t know why the surgeon general insists the COVID jab offers better protection against variants than natural immunity. I don’t see how it could. The lack of rational medical explanation is suspicious, and perhaps that’s why 40% of the American population has yet to take the jab.34
- 1 MSN August 17, 2021
- 2, 4 CDC MMWR August 13, 2021; 70(32): 1081-1083
- 3 CDC.gov August 6, 2021
- 5 Our World in Data, Data for Israel
- 6 David Rosenberg 7 July 13, 2021
- 7 Sharylattkisson.com August 8, 2021
- 8 Sharylattkisson.com August 6, 2021
- 9 Twitter Alex Berenson July 18, 2021
- 10 The New York Times July 16, 2021
- 11 Bloomberg COVID Vaccine Tracker
- 12 Mayo Clinic COVID Vaccine Tracker
- 13 Medicina 2021; 57: 199
- 14 The Lancet Microbe July 1, 2021; 2(7): E279-E280
- 15 Annals of Internal Medicine September 2, 2020 DOI: 10.7326/M20-5352
- 16 BBC News July 14, 2021
- 17 FBA News August 9, 2021
- 18 NBC News August 7, 2021
- 19 US District Court of Alabama Civil Action No. 2:21-cv-00702-CLM (PDF)
- 20 The Defender July 20, 2021
- 21 Open VAERS
- 22 NPR February 19, 2021
- 23 Nature Medicine March 16, 2021; 27: 569-570
- 24 Cell May 14, 2020 DOI: 10.1016/j.cell.2020.05.015
- 25 Wall Street Journal June 12, 2020 (Archived)
- 26 Medrxiv DOI: 10.1101/2020.04.17.20061440
- 27 Biorxiv preprint DOI: 10.1101/2020.05.26.115832 (PDF)
- 28 Daily Mail June 12, 2020
- 29 Science Times June 12, 2020
- 30 Geert Vanden Bossche, DMV PhD Open Letter
- 31 MMWR December 18, 2020
- 32 Full Measure After Hours Podcast January 30, 2021
- 33 Full Measure News January 31, 2021
- 34 Mayo Clinic COVID Vaccine Tracker, as of 8/18, 60.1% have received 1 dose





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr