Analysis by A Midwestern Doctor
STORY AT-A-GLANCE
- The Cell Danger Response is an evolutionarily conserved adaptation cells use to protect themselves from environmental stressors
- Mitochondria orchestrate the CDR by first detecting a threat and then switching from powering the cell to shutting it down to protect the cell from danger. Many complex illnesses result from a chronically sustained CDR that prevents the cells from their normal functionality
- Therapies which address the CDR are often necessary to treat a variety of complex illnesses such as chronic fatigue syndrome, autism, and COVID-19 vaccine injuries
Since early 2020, I have worked with patients with spike protein injuries, either from COVID-19 or the vaccines. Now and then, I’ve observed a specific treatment for a spike protein injury have a rapid effect that was so dramatic it would have been difficult to believe it had happened had I not witnessed it firsthand.
Whenever I spotted a treatment doing that, I asked, “Why did this happen?” Over time, I realized two mechanisms appeared to be able to account for almost every case where I observed this happen.
The first was that impaired fluid circulation in the body was restored, most commonly by restoring the physiologic zeta potential (something the spike protein is uniquely suited to inhibit). Since this is a complex but relatively unknown topic, I’ve worked to explain what zeta potential is, how its disruption creates illness by impairing fluid circulation throughout the body, and the methods I know of which can restore it.
Note: In parallel to doing this, I also discussed the fourth phase of water (something also critical for the health of the body) as the two concepts are deeply interrelated.
The second was that the Cell Danger Response (CDR) was deactivated. Since there is much more awareness about this (still relatively unknown) concept in the integrative medical field, I felt zeta potential needed to be covered first. Nonetheless, the CDR is an essential concept to understand, and like zeta potential, it plays a foundational role in explaining and addressing many of the complex conditions we face today.
Before I go further, I would like to acknowledge two of my colleagues who have a great deal of experience working with the CDR that assisted me in drafting this series (and both independently observed that the COVID vaccines triggered the CDR).
What Is the Cell Danger Response?
For cells to survive, something has to protect them from the innumerable threats they encounter. In complex organisms, we typically assign that role to the immune system. In contrast, in single-celled organisms (e.g., bacteria), it’s fulfilled either by them putting protective agents into their environment (e.g., bacteriocins to kill enemy bacteria) or them evolving resistance to the danger they are facing (e.g., antibiotics).
However, those are not the only options. In a previous article where I tried to explain the potential consequences of bacteria DNA being found in the vaccines, I touched on an important concept. When bacteria (and fungi) are placed in a dangerous environment, in addition to those that die, some will transform into a form better suited to survive the hostile environment (this is the most well-recognized with spore-forming bacteria).
Note: Since those forms are often more likely to cause diseases and resist antibiotics, it can be counter-productive to continue addressing them with the same antibiotics, and different approaches are needed to aid patients with those infections.
When cells are stressed by their environment, they also transform into a more defensive state primarily mediated by the cell’s mitochondria (which are essentially bacteria and able to rapidly adapt to changes in their environment). This process has been observed by many (e.g., some call it the integrated stress response), and I believe the process is the most comprehensively described by the CDR.
The CDR concept is frequently credited to Robert Naviaux (someone I consider a genius). He integrated all of the existing scientific knowledge on cellular adaptations, utilized a variety of established approaches (e.g., genomic analysis), and, most importantly, used an innovative but relatively unknown diagnostic method, metabolomics, to map out the CDR.
Metabolomics uses mass spectrometry to identify every biomolecule present in a sample of blood, which is both quite feasible and provides an in-depth understanding of the body which, to my knowledge, cannot be obtained with any other existing technology (e.g., the endless lab tests that provide a narrow snapshot of the body which may not have any correlation to the patient’s symptoms). This is how Naviaux described the merits of the technology:
“First, fewer than 2,000 metabolites constitute the majority of the parent molecules in the blood that are used for cell-to-cell communication and metabolism, compared with 6 billion bases in the diploid human genome. Second, metabolites reflect the current functional state of the individual. Collective cellular chemistry represents the functional interaction of genes and environment.”
The process of the CDR essentially is as follows:
1.Something stresses the cell.
2.Mitochondria within the cell rapidly detect this stress (e.g., before the stressor can kill the cell). This detection, Naviaux argues, is due to electrons that previously were available to mitochondria being diverted to the stressor (e.g., an invading virus hijacking the cell to reproduce, a heavy metal being present, or many of the harmful [electron stealing] chemicals we are exposed to now), which creates a voltage drop in the mitochondria.
3.The mitochondria then reduce or terminate their primary function (creating energy in the form of ATP for the cell) and switch from an anti-inflammatory to a pro-inflammatory state (macrophages also switch from an anti-inflammatory to a pro-inflammatory form).
4.Because the mitochondria producing ATP uses up a lot of oxygen, once that production is reduced (or becomes incomplete) and the mitochondria shift to producing different biomolecules, the available oxygen in a cell rapidly increases. For context, mitochondria contain 1500 proteins tailored to meet the needs of each cell type and catalyze over 500 different chemical reactions in metabolism.
These mitochondrial effects (particularly the elevated oxygen) cause the following to occur:
| Production of complex proteins (polymers) is reduced, which viruses require to reproduce. | Protective changes in the behavior of the whole organism (e.g., increased tiredness that induces the sleep needed to facilitate healing or a desire to isolate so the infection is not transferred to other members of their group). |
| Antiviral and antimicrobial substances are released inside the cell. | Warning cells in the vicinity that a danger is present. |
| Increased consumption (autophagy) of components within the cell, including the defective parts of the mitochondria and the mitochondria themselves. | Changes in gene expression and mobilization of parts of cellular DNA. |
| The cell membranes stiffen so things are prevented from passing through it. |
Note: A long time ago, a mentor versed in some of the most remarkable forgotten sides of medicine showed me an ancient test his teacher used to evaluate if the body was consuming oxygen properly (something they believed was critical for proper health). The test was known as the blood crenation test and assessed the degree to which cells would change their size once placed in a hypertonic solution.
After I learned about the CDR, I realized that the test detected if the membranes had stiffened due to an active CDR and mitochondria, in turn, not correctly consuming oxygen. That stiffening is greatest during CDR1 and begins to soften during CDR3 (explained below).
I found this fascinating because the therapy (designed to treat numerous illnesses through restoring the oxidative metabolism of cells) he used the blood crenation test for had two stages of treatment, and the second stage could only be used once the first stage had sufficiently softened the cell membranes.
In the recent series on zeta potential, I argued that a key reason for why zeta potential disruption has become a root cause of so many illnesses is due to the physiologic mechanisms for maintaining zeta potential having evolved in an era where the human body faced far fewer zeta potential disrupting toxins.
Because of this, the baseline zeta potential our body is designed to maintain (keep in mind that an excessive zeta potential also creates problems) is often not strong enough to counteract those harmful environmental influences.
The CDR likewise evolved in an era when humans faced far fewer stressors and is not appropriately calibrated for the modern world. For example, when the CDR is activated, the oxidizing environment causes cells to sequester rather than excrete heavy metals. This is a problem since heavy metals (which are now common in our environment) are both a common cause of chronic illness and a trigger for the CDR.
When Naviaux originally mapped the CDR out, he thought that it had one phase, but in time realized it had three different phases, the initial response, a proliferative phase (which rebuilds tissue), and then the cell beginning to return to its initial function:
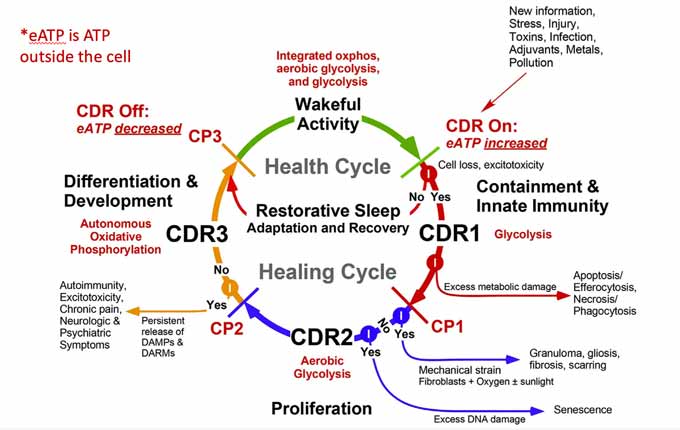
Naviaux’s central argument is that while the CDR is a normal adaptive response, it will create problems if cells get stuck in one of the CDR phases because they did not receive the final all-clear signal to exit the CDR.
Note: Chronic diseases are characterized by impaired communication between cells and tissues. If this occurs at a young age (e.g., in autism), the normal trajectory of development is altered, leading to the abnormal tissue and organs the body’s systems must adapt to. In adults, these alterations cause tissue and organ performance to degrade over time, eventually leading to various problems such as cancers and organ failures.
During CDR2 (which, amongst other things, Naviaux links to cancer), dividing and migrating cells cannot establish long-term metabolic cooperation between cells because their location within tissues is continuously changing. CDR3, in turn, is the integration phase that allows cellular communication to be restored, and hence is critical to complete for many complex illnesses.
Additionally, CDR3’s completion is aided by the autonomic nervous system being in a rest and recovery state (facilitated by the vagal nerve — the parasympathetics are one of the foundational ways to communicate safety to the body).
My colleagues believe this helps to explain why the converse, excessive stress, and sympathetic activity that characterizes the modern age can have such a large impact on chronic illnesses, as they signal to the body danger (that requires a CDR) is still present.
What Are the Effects of the CDR?
Much of this series was an attempt to simplify and summarize Naviaux’s years of research. The specific publications I referenced throughout this article were as follows:
| The original 2014 paper which explained the CDR. |
| A 2016 study of patients with chronic fatigue syndrome (CFS) identified consistent patterns within their metabolomics. Those hypometabolic changes resembled dauer, an evolutionarily conserved state organisms enter that makes them much more capable of surviving environmental stressors and conserving energy but much less able to engage in normal activity (e.g., a functional life free of suffering and disability).
Since the biological clock within those cells slows (and they can survive periods of resource starvation), they can outlast the cells that fail to make this transition and take over once conditions are safe for the cells to return to normal. Note: Many of the genes involved in dauer have been actively studied for promoting longevity (e.g., they overlap with the changes created through caloric restriction). Additionally, in dauer, behavioral responses become “brittle,” such that small stimuli produce significant responses in otherwise docile animals, a phenomenon also commonly observed in complex chronic illnesses. |
| A pilot 2017 study where autistic children were provided a CDR blocking agent. This double-blind trial demonstrated significant improvement in autistic children, which to my knowledge, has not been obtained in any other clinical trial attempting to treat autism. |
| A 2017 review of the cell danger response and the potential applications in using CDR targeting agents for conditions such as autism. |
| A 2018 paper discusses the CDR’s three stages and how they are part of the body’s normal healing cycle. This is the most detailed overview of the CDR Naviaux has written and the paper I most recommend reading. |
| A brief 2020 paper connecting the CDR to mitochondrial dysfunction and chronic illness. |
| A 2020 study evaluated the link between viral infection and the CDR. It found the HHV-6 virus (to which 90% of the population is exposed by age three) could trigger the CDR.
Once activated, the CDR shielded cells from other viruses as there was up to a 99% decrease in their infection from influenza or HSV-1. Notably, the CDR persisted even when HHV-6 was almost undetectable, and serum from CFS patients could induce the CDR within healthy cells (and matched the CDR seen in CFS), thus demonstrating that a pathologic CDR can persist long after the inciting stimulus disappears. |
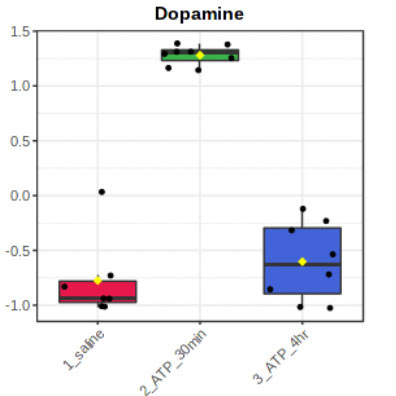
| A 2021 study exposed rats to the primary CDR-inducing agent (ATP) and then measured the metabolic and behavioral changes that followed (e.g., whole body oxygen consumption decreased by 74% and rectal temperature dropped by 6.2?C in 30 minutes — both of which are massive changes).
This paper is the most detailed published study (I know of) that has been conducted on how the CDR alters both behavior and biochemistry (over 200 metabolites from 37 different biochemical pathways were changed). Furthermore, it found that most of the changes returned to baseline in a few hours and that the responses in male and female rats to ATP were noticeably different (males were more sensitive to behavioral changes, females were more sensitive to metabolic changes). |
| A 2023 review paper that discussed the current understanding of the CDR and methods for treating it. Much of this paper is discussed in the third part of this series. |

Download this Article Before it Disappears
Purinergic Signaling
The primary agent that appears to set off the CDR is ATP leaking out of cells (which evolutionarily makes sense as its concentration is approximately one million times higher inside cells compared to outside them, so it will consistently leak out when the cell is damaged or stressed).
In addition to this leak occurring due to damage to the cell, there are also redox-gated, mechanical stress-gated and voltage-gated channels that directly facilitate this leak alongside ATP exporting vesicles, all of which allow one cell in the CDR to induce the CDR within the cells surrounding it through purinergic signaling.
In turn, ATP (a purine) and a variety of related molecules (that often leak in tandem with it) are detected by numerous receptors throughout the body, affecting them through a process known as purinergic signaling. Since purinergic signaling is a relatively new field of study, each year, more and more of its implications for the body are being discovered (e.g., its role in the communication between cells, the stress response, autonomic, vestibular, and many sensory integration pathways).
Many of the consequences of the CDR result from the changes created within the nervous system. ATP or its metabolites have also been found, according to Naviaux, to “be co-neurotransmitters and neuromodulators at every synapse in the central and enteric nervous systems, and every immunologic synapse that has been studied to date.”
Purinergic receptors control neurotransmission, cortisol production, inflammation, chronic pain signaling, and autonomic nervous system control.
Furthermore, Naviaux has proposed that the effects of CDR purinergic signaling help explain why the human body responds to danger by exhibiting the stereotypical behaviors observed in sickness (e.g., during the flu or while recovering from a severe injury), such as withdrawing from social contact, decreasing speech, having fragmented sleep, or developing an increased sensitivity to heat, touch, sound, and light.
For example, in the rats studied, triggering the CDR caused them to decrease their motor activity, avoid open areas (or explore new ones) and to develop gait coordination abnormalities. The presence of purinergic receptors at neural synapses has also implicated purines as being a necessary component of learning.
In conjunction, the 2021 study showed activating the CDR spiked the levels of dopamine in the body (a key neurotransmitter for learning and creating habits within the nervous system).
It is frequently observed that if an injury (e.g., a head concussion) occurs before a previous version of the same injury finishes healing, the consequences of second injury (even if much lighter) can be significantly greater than the original injury.
Similarly, is known that stimulating the immune systems of pregnant mice (in a process mimicking what a viral infectious would do) increase the likelihood of offspring with features resembling those seen in neurodevelopmental disorders such as autism or in schizophrenia. In the 2021 study, when that same stimulation was done to pregnant mice, their offspring became hypersensitive to the effects of injected ATP and took much longer to return to their baseline.
Two of the greatest challenges in treating patients with a complex chronic illnesses are their susceptibility towards relapses (e.g., one triggered by a light stressor) and the body becoming programmed to have something akin to an addiction to the chemicals released by the CDR (e.g., the risk of a recurrence of depression is 3-6 times greater than the risk in those who have not previously been depressed). Lastly, to quote Naviaux:
“Complex negative and maladaptive behavioral responses to adversity can be paradoxically reinforced by an anti-inflammatory effect they produce at the cellular level.”
Because of all of this, many of my colleagues suspect that the CDR triggers a learning process that causes patients to become progressively easier to trap in a CDR state each time a successive threat is presented toward them, even when the original trigger or stressor is no longer present.
This is a major reason why the proper treatment of a chronic illness often requires recognizing the body’s existing momentum towards illness and incomplete recovery, and then gradually redirecting it to wellness.
Note: I also believe impaired lymphatic drainage from the brain helps to account for the severity of successive concussions.
Why Is the CDR Important?
One of the major problems we face in medicine is the immense amount of data available to us and our simultaneous inability to integrate it into a coherent story that makes sense for patients. For example, functional medicine practitioners memorize an endless number of biochemical pathways. However, in many cases understanding why so many different pathways can be abnormal is only possible with the context provided by the CDR.
Additionally, many apparently harmful genetic variations (polymorphisms) are frequently assessed and then mitigated by functional medicine practitioners. The CDR often provides a critical context for why these variations exist, as when the CDR is active, unexpected benefits can arise from the presence of the “defective” polymorphism.
One colleague (an integrative physician and leader in the discipline) who frequently uses the CDR in clinical practice feels it is invaluable because the CDR helped them understand why integrative therapies they thought should work never did anything for patients (and sometimes harmed them).
For example, as the years have gone by, the medical field (particularly within integrative medicine) has tied more and more chronic diseases to mitochondrial dysfunction and treated them with supplements (or energy-inputting therapies) designed to increase mitochondrial output. This works if the issue arises from a deficiency of what the mitochondria need but does not help if the decreased mitochondrial output is instead a protective adaptation.
In some cases, this means the patient wastes money on unneeded supplements, and in other cases (e.g., sometimes with intravenous NAD), the patient can feel quite bad afterward if parts of their system were not ready for the mitochondrial function to be upregulated. This harmful reaction commonly occurs if the agent inciting the CDR is still present but treatments are instead directed at negating the symptoms created by an active CDR.
Note: In the rat study, triggering the CDR did not deplete the levels of any vitamin.
Since the CDR is such a fundamental survival mechanism, the changes in metabolism, inflammation, immunity, microbiome, brain function, sleep patterns, and social behaviors the CDR creates can be triggered by many different kinds of threats (e.g., infection, pollution, poisoning, physical or psychological trauma, a lack of nutrients or blood to the cells and even a reduced gravity environment).
Within the 2016 study on 45 CFS patients, for instance, over a dozen triggers for CFS were identified, with some patients having multiple triggers occurring in the same period, and no trigger being significantly more common than the rest.
Note: Frequently in complex diseases, patients pass a critical threshold of (highly variable) stressors, and then have a radically altered physiology which becomes dramatically more sensitive to additional stressors.
Conversely, because the CDR can get stuck in different phases (creating different types of diseases) and often only affects specific cells within the body (e.g., only a particular tissue or some but not all the cells within one tissue) it is thus possible to have the same underlying process cause an immense number of seemingly different diseases.
Note: Naviaux’s best attempt to map many of the common chronic diseases to a CDR phase can be found here in Table 1. For example, a defining characteristic of CFS and often fibromyalgia is an inability of the body to replenish its energy after exertion (or sleep). This makes sense if mitochondria are producing much less of the ATP needed for that energy replenishment and some of the ATP they produce is leaking out of the cell.
Within our linear scientific paradigm, every cause must be attributed to one effect. This leads many to be at a loss in understanding how so many different things can cause the same inexplicable illness. Furthermore, since many believe scientific proof requires a repeatable cause and effect relationship, it is almost impossible to convince skeptical audiences of the legitimacy of these non-linear conditions.
Thus, without a unifying model like the CDR that accounts for this immense variability, there are myriad of “complex” diseases that are nearly unsolvable within the existing paradigm. For example, to quote Naviaux:
“Complex [multisystem] diseases like CFS are often difficult and expensive to diagnose [e.g., no single diagnostic test yet exists for CFS].
Although individual tests may be affordable and possibly covered by medical insurance, many patients undergo a diagnostic odyssey that results in substantial personal expenditures that can exceed $100,000 over years of searching [for a cure], absence from the workplace, and significant reductions in quality of life.”
Naviaux’s 2016 words describe exactly what countless COVID vaccine injured individuals have also experienced. One of these patients, for example, had seen 31 doctors before me (many of whom worked at prestigious institutions) and felt only two of them (both of whom had already left the conventional system) could provide anything helpful. The rest ordered various expensive tests that were mostly covered by insurance but provided no benefit whatsoever to the patient.
As another example, the national economic cost of autism is estimated to be $75,000 per patient with autism, and the average family caring for a family member with autism, in turn, spends over $17,000 on necessary care expenses not covered by public services. Since the incidence of autism is rapidly growing, this cost is growing too (it reached $268 billion in 2015 and is expected to rise to $461 billion by 2025).
Note: I previously reviewed Peter Hotez’s book that argued vaccines do not cause autism (without providing anything to substantiate his claim). Hotez’s justification for frequently attacking parents who link vaccines to autism was that doing so diverts public funding away from supporting the out-of-pocket expenses parents like Hotez have to spend caring for autistic children.
Given the rate at which autism is rising within the USA, that is a nonsensical approach akin to scooping water out of a boat with a large hole in the hull.
Because of the economic impact of autism, over $1 billion has been spent on research for the genetic causes of autism over the past ten years. This work has shown that hundreds of genes play a role in different children and that no single gene accounts for more than 1–2% of autism.
Conversely, other politically unpalatable causes (e.g., multiple vaccinations in close succession activating the CDR or other environmental stressors that can as well) are never looked at. Similarly, viable treatments that have both a mechanistic basis and clinical evidence to support them, but are not profitable (e.g., Naviaux used a repurposed drug to treat autism), are sadly never looked at.
This situation is virtually identical to what I previously discussed with the even more impactful condition, Alzheimer’s disease. Billions are spent each year on (sometimes fraudulent) research that has relentlessly focused upon a highly questionable mechanism for the disease that has consistently failed to produce a viable therapy for the disease.
Conversely, proven treatments based on different models of the disease exist, which very few Alzheimer’s researchers are even aware of.
Like Naviaux, I feel the lack of treatments for autism is particularly tragic because autistic children are often highly gifted individuals, and I have seen numerous cases of an autistic child who was cured (or at least significantly improved) with an “unproven” treatment that then went on to lead an immensely impactful and productive life.
Unfortunately, those treatments are rarely available; instead, many autistic children are often treated terribly (e.g., they experience a very high rate of physical or sexual abuse), and what they go through is almost invisible to those who do not directly work with them. Similarly, many older adults with dementia are often treated quite poorly, but placed in areas like nursing homes where they can be kept out of sight and out of mind.
What I find so surprising about Naviaux’s work is its commercial potential (as numerous drugs which inhibit purinergic signaling improve conditions linked to the CDR).
However, despite the fact Naviaux has meticulously laid out all the research that demonstrates the importance of the CDR for over a decade, his work has not caught on outside the alternative medical field, and no pharmaceutical company has seriously pursued developing drugs targeted at the numerous purinergic receptors throughout the body.
Why Do Spike Proteins Set off the CDR?
Presently, I believe there are three causes for most of the symptoms individuals experience with spike protein injuries:
- Circulatory obstructions
- Autoimmunity
- Immune suppression
It turn, I’ve tried to put forward some of the mechanisms that could be causing these to happen. For example, I believe the circulatory issues are due to the spike protein damaging the protective lining of the blood vessels, the spike protein creating misfolding within the proteins the body uses to create fibrin clots, and as mentioned above, the spike protein collapsing the physiologic zeta potential of the body. In regards to autoimmunity, I have thus far proposed that the primary issues are:
- The spike protein being inherently immunogenic (stimulating to the immune system).
- The spike protein having a highly unusual degree of overlap with human tissue.
- Vaccines being designed so that the immunogenic spike protein is expressed on the surfaces of cells.
Additionally, I also believe the spike protein’s effects on zeta potential exacerbate this issue.
Note: Because spike proteins overload the cells, many find their way to the cell surface. In addition to triggering the immune system to destroy the spike protein-expressing cell, it also causes parts of the membrane to separate from the cell and travel through the body as exosomes.
The body relies upon exosomes for communication between the cells (including to signal the CDR), and spike protein-coated exosomes have been detected in mRNA-vaccinated individuals.
The changes in the exosomes throughout the body have been both hypothesized to account for many of the pathologic changes observed in these patients and to explain how the seemingly impossible mRNA vaccine shedding can occur (as exosomes are also exhaled); presently, the only other potential mechanism I have identified to explain the inexplicable shedding process is bacterial DNA within the vaccines causing the microbiome to express the spike protein.
A key feature of the CDR is the mitochondria transforming from their typical energy-producing state to a pro-inflammatory state that activates the innate immune system. Thus, in addition to fatigue and varying degrees of organ dysfunction arising in individuals whose mitochondria are no longer devoted to powering the cells, a wide range of inflammatory conditions (e.g., autoimmune disorders) can result from a sustained CDR (e.g., that caused by an infection like HHV-6).
Conversely, many of my colleagues have also observed that the same therapy which we have found rapidly treats the CDR in spike protein injured patients (i.e., acute covid, long covid, and covid vaccine injuries) also can treat challenging autoimmune disorders (e.g., Sjögrens syndrome) in patients not suffering from spike protein injuries.
Likewise, before COVID-19, my colleagues who specialized in complex autoimmune conditions frequently found approaches they believed targeted a persistent CDR simultaneously improved many of the autoimmune disorders those patients were suffering from.
One of the biggest things that have helped my team develop treatments for spike protein vaccine injuries is that many of the modes of harm we’ve witnessed from these injections resemble what we had previously seen with other vaccines.
The big difference is that the toxicity and rate of adverse events from the COVID-19 vaccines are much higher than that seen with a typical vaccine, so certain reactions (e.g., sudden deaths in healthy adults) are unique to this vaccine, and its harms are frequent enough the general population can recognize them.
Previously, I advanced Andrew Moulden’s argument that every vaccine causes harm due to their effects on the physiologic zeta potential (along with the immune system further obstructing circulation by having its large cells enter the smallest vessels of the body).
The easiest way to detect these circulatory obstructions is from the pathological changes the microstrokes create, and I have noticed many of my vaccinated friends developed the same neurological signs Moulden observed in vaccine-injured children (e.g., an eye’s ability to move outward becomes impaired).
Vaccinations, likewise, are well suited to activating the CDR. Typically, when the body confronts an invader, it is dealt with on its surface (e.g., within the respiratory mucosa), and a specific immune response is created to address it. It is much rarer for the body to first confront an invader within the bloodstream.
When this occurs, the cells sense a greater danger, and a much more severe response is directed toward the invader that rarely prevents the initial stages of an infection that mucosal immunity typically prevents.
Since vaccines that use the natural routes of exposure that trigger the body’s first line of defense are harder to develop (the oral polio vaccine being one of the only examples), we typically default to vaccinations that utilize a backdoor into the immune system that instead activates its final line of defense. This amongst other things causes different antibody types to be produced by the system.
Furthermore, we often repeatedly administer the same vaccine (and multiple vaccines simultaneously), thereby providing a repeating stimulus that trains the CDR to become progressively easier to activate.
Sadly, due to the widespread blind faith in the safety and efficacy of vaccines, basic practices to improve their safety (e.g., spacing them out), let alone their effects on the CDR and zeta potential, rarely, if ever, enter the conversation. Furthermore, outside of Naviaux’s circle, very few are even aware that activating the CDR plays a key role in how the body develops immunity to a foreign entity.
In addition to the inherent toxicity of the spike protein, the mRNA vaccines design itself is particularly well suited to triggering the CDR. Because the mRNA is designed to transfect cells, like an actual viral infection, it continually steals the resources of the cell to manufacture the synthetic spike protein, and like what occurs in a viral infection, the mitochondria most likely detect this theft and initiate the CDR.
There are also many other issues with overstimulating the body’s immune response. For example, to quote the National Cancer Institute:
“[T cell exhaustion] describes a condition in which T cells (a type of immune cell) lose their ability to kill certain cells, such as cancer cells or cells infected with a virus [or mRNA spike proteins]. This can happen when cancer, chronic infection, or other conditions cause the body’s immune system to stay active for a long time.
Exhausted T cells have high amounts of immune checkpoint proteins on their surface, which may keep the activity of the T cells suppressed [as excessively killing the cells of the body is also dangerous and must have a counterbalance to prevent it from occurring]. In cancer treatment, drugs that target these proteins may be given to allow the T cells to better kill cancer cells.”
T cell exhaustion is one of the many issues that must be addressed when working with complex illnesses (e.g., this frequently comes up with chronic Epstein Barr infections — a dormant condition that many have reported reactivates in vaccine-injured patients).
One of the interesting things my colleagues have found is that T cell exhaustion is also commonly observed in patients with long covid and spike protein vaccine injuries (which my colleagues also suspect is what triggers the Epstein Barr reactivation).
Lastly, beyond reducing the cell’s ability to produce proteins, the CDR also triggers the cell to degrade the foreign material within it. Unfortunately, to make the mRNA vaccines “work,” their mRNA was modified through pseudouridation to resist degradation so the mRNA could produce the spike protein for a much longer period within the cell — which unfortunately leads to the mitochondria repeatedly being signaled to initiate the CDR.
At this point, it is still unknown why stressors (e.g., mounting an immune response to an invader) cause some individuals to develop a permanent rather than temporary CDR; the only thing that is known is repeated activations of the CDR make it more likely to become permanent.
Note: In the 2021 rat study, briefly triggering the CDR was shown to initially either increase or decrease a wide range of metabolites in the body, with the metabolites returning to their original levels in a few hours. One of the few exceptions to this rule was pseudouridine, which initially had a slight increase, but over time, rather than returning to baseline, developed a much more significant increase.
This pseudouridine elevation might be one of the mechanisms at work in vaccine injury (e.g., pseudouridated mRNA is thought to suppress the immune system), however, I do not know of a study that has directly assessed if pseudouridine levels become elevated following mRNA vaccination, particularly within chronically ill patients who appear to be trapped within the CDR.
Conclusion
My sincere hope is that this series, along with the previous one on liquid crystalline water and zeta potential, has helped to provide a framework to explain the perplexing question of why numerous stressors (e.g., toxins) can cause the same disease and why the same stressor can create such a widely varying spectrum of illness in those exposed to it.
I have done my best to accurately simplify this subject, and regrettably, despite all the work I’ve done thus far, I still feel I have only scratched the surface of that perplexing question. For example, I am frequently asked about the relationship between the CDR and zeta potential or liquid crystalline water. The short answer is that I know they are interrelated as:
- The CDR goes hand in hand with fluid stagnation (each exacerbates the other—for example interstitial pressure, a sign of obstructed fluid circulation, increases in CDR1).
- One of the changes observed within cells during the CDR is a destructuring of the liquid crystalline water within it (discussed further by Naviaux here)
- That ATP is concentrated in the liquid crystalline water layer which surrounds each cell (and likely plays a key role in creating that layer).
The major challenge with the current understanding of the CDR is how to treat it. On the one hand, to some extent, countless therapies can help (e.g., now that the CDR is known about in parts of the integrative medical community, patients and colleagues periodically introduce me to natural preparations that allegedly treat it).
However, creating a consistent improvement in the CDR is much more challenging and requires both targeted treatments and a comprehensive understanding of the CDR.
Fortunately, one medical specialty, regenerative medicine, emphasizes restoring the critical functions of non-functional tissue. Because of this, the field has independently developed a comprehensive understanding of why cells get trapped in a non-functional state and the most direct ways to restore their functionality.
In the next part of this series, I discussed the practice of regenerative medicine and its perspectives in treating the CDR. This helps to lay the context for the final part of the series on the methods within the integrative medical field and the regenerative medical field that treat the CDR, and that we have seen help numerous individuals with spike protein injuries recover from their illness.
Lastly, it should also be noted that in the same way I have previously characterized many of the diseases of aging as being partly due the physiologic zeta potential worsening with ago (likely resulting for a declining kidney function), the CDR also worsens with age.
Hence, many of the effects arising from a sustained CDR that were described throughout this article, will to varying extents eventually be seen in everyone and thus are something the regenerative medical field has prioritized finding ways to address.
A Note From Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician in the Midwest and a longtime reader of Mercola.com. I appreciate his exceptional insight on a wide range of topics and I’m grateful to share them. I also respect his desire to remain anonymous as he is still on the front lines treating patients. To find more of AMD’s work, be sure to check out The Forgotten Side of Medicine on Substack.





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr