Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- At the end of December 2022, John Campbell, Ph.D., posted a video calling on the British health authorities to halt the use of mRNA COVID injections, as the data suggest there are far too many safety issues
- Campbell argues that while the risk of complications and death due to COVID has significantly lessened since the early days of 2020, the risks associated with the COVID jabs remain the same. Hence, the risk-benefit ratio of the mass injection campaign has flipped, and the risk associated with the shot now outweighs the risk of infection
- The COVID jabbed are now dying in greater numbers than the unjabbed — so much so that it has driven down the overall life expectancy in the U.S. by nearly three years
- Across the world, excess mortality has dramatically risen since the rollout of the jabs. If they were beneficial, you’d expect excess mortality to drop. We’re also not seeing mass death from COVID. The only clear factor that might account for these discrepancies is mass injection with an experimental gene transfer technology
- Most COVID-19 related deaths are also occurring among the fully jabbed and boosted
Since the beginning of the COVID pandemic, John Campbell, Ph.D., a retired nurse educator, has gained a following for his even-handed evaluations of COVID science and statistics. While he’s not known for taking a stand against the COVID shots, that recently changed.
At the end of December 2022, Campbell posted a video (above) calling on the British health authorities to halt the use of mRNA COVID injections, as the data suggest there are far too many safety issues to continue.
Moreover, most COVID-19 hospitalizations in 2022 were incidental, meaning they were not hospitalized “for” COVID but, rather, tested positive once admitted. Waves of outbreaks with newer, less hazardous variants have also resulted in high levels of natural immunity.
Campbell argues that while the risk of complications and death due to COVID has significantly lessened since the early days of 2020, the risks associated with the COVID jabs remain the same as they were at the outset.
Hence, the risk-benefit ratio of the mass injection campaign has flipped, and the risk associated with the shot now outweighs the risk of infection. Campbell is now urging the British government to pause the continued booster campaign until a population-wide risk-benefit analysis has been carried out, and the data published with full transparency so that independent researchers can verify the findings.
Life Expectancy Plummeted After COVID Jabs Rolled Out
What Campbell does not address in this video, but has reviewed in others, is that the COVID jabbed are actually dying in greater numbers than the unjabbed — so much so that it has driven down the overall life expectancy in the U.S. by nearly three years.1
In 2019, the average life span of Americans of all ethnicities was 78.8 years.2 By the end of 2020, it had dropped to 77.0 years3 and by the end of 2021, it was 76.4.4
We know this drop isn’t due to people dying of COVID-19, because the age groups with the highest increases in mortality were working age adults, 25 through 54, followed by children between the ages of 1 and 4.5 And, they are not tiny increases.
Rates of death increased 16.1% for 35- to 44-year-olds, 13.4% for 25- to 34-year-olds, 12.1% for 45- to 54-year-olds, and 10.1% for 1- to 4-year-olds. Meanwhile, COVID mortality was, from the start, highest among the elderly.
The average age of death due to COVID-19 was 82,6 which is actually older than the average life span, and mortality rates only increased by 3.8% among 65- to 74-year-olds and 2.4% among those aged 75 to 84. Life insurance data also confirm that it’s working age adults who are dying in record numbers.7
Excess Mortality Took Off After COVID Shots Were Introduced
COVID-19 is also an unlikely cause for the rapid decline in life expectancy for the simple fact that it’s not a major contributor to rising excess mortality, which only took off after the introduction of the COVID shots in early 2021.8
Excess mortality is a statistic that is related to but separate from life expectancy. It refers to the difference between the observed numbers of deaths (from all causes) during a given time, compared to the expected number of deaths based on historical norms, such as the previous five-year average. (Formula: reported deaths – expected deaths = excess deaths.)
Across the world, excess mortality has dramatically risen since the rollout of the jabs, and barely a day now goes by without a healthy adult suddenly dropping dead with no apparent cause.
If the COVID jabs were beneficial, you’d expect excess mortality to drop, yet that’s not what we’re seeing. We’re also not seeing mass death from COVID. The only clear factor that might account for these discrepancies is mass injection with an experimental gene transfer technology.
The Jabbed Also Account for Most COVID-19 Deaths
U.S. Centers for Disease Control and Prevention data also show that most COVID-19 related deaths are now occurring among the jabbed and boosted, and this despite the fact that numbers are artificially suppressed by only counting people as “vaccinated” or “boosted” if they’re at least two weeks out from their last shot. As reported by the Kaiser Family Foundation (KFF):9
“In fall 2021, about 3 in 10 adults dying of COVID-19 were vaccinated or boosted. But by January 202210 … about 4 in 10 deaths were vaccinated or boosted. By April 2022 … data11 show that about 6 in 10 adults dying of COVID-19 were vaccinated or boosted, and that’s remained true through at least August 2022 (the most recent month of data).”
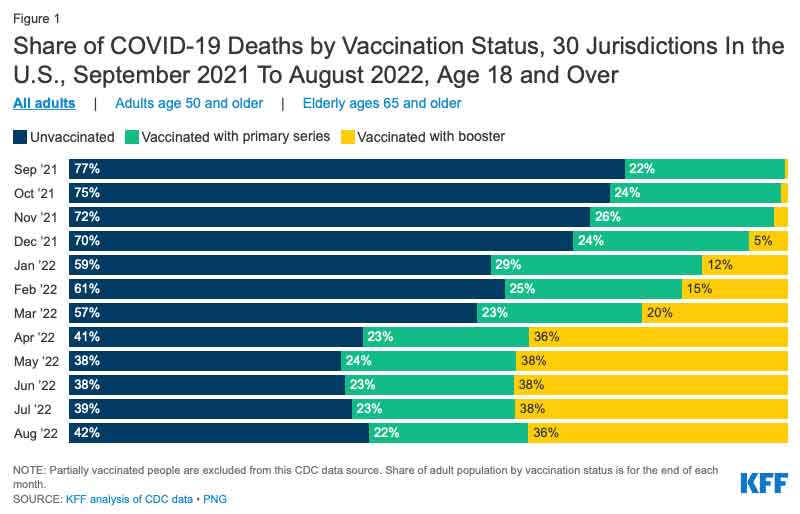
The data from this chart come from the CDC, which collects data on the number of deaths by vaccination status from 30 health departments (including states and cities) across the country.
In order to be counted as vaccinated, a person must be at least two weeks out from completing their primary series … Similarly, to be counted as having a booster, a person must be at least two weeks out from their booster or additional dose before testing positive. People who were partially vaccinated are not included in this data.”
COVID Jab Is Likely Fueling Mutation of Variants
Another reason to halt the COVID booster campaign that Campbell does not address is the very likely possibility that the shots are fueling mutations, giving rise to ever new and more resistant variants. As reported in a Wall Street Journal opinion piece by Allysia Finley,12 “The virus appears to be evolving in ways that evade immunity,” which is bad for the jabbed and unjabbed alike.
“Public-health experts are sounding the alarm about a new Omicron variant dubbed XBB that is rapidly spreading across the Northeast U.S.,” Finley writes.
“Some studies13 suggest it is as different from the original COVID strain from Wuhan as the 2003 SARS virus … It isn’t clear that XBB is any more lethal than other variants, but its mutations enable it to evade antibodies from prior infection and vaccines as well as existing monoclonal antibody treatments.
Growing evidence also suggests that repeated vaccinations may make people more susceptible to XBB and could be fueling the virus’s rapid evolution …
Under selective evolutionary pressures, the virus appears to have developed mutations that enable it to transmit more easily and escape antibodies elicited by vaccines and prior infection.
The same study posits that immune imprinting may be contributing to the viral evolution. Vaccines do a good job of training the immune system to remember and knock out the original Wuhan variant. But when new and markedly different strains come along, the immune system responds less effectively.
Bivalent vaccines that target the Wuhan and BA.5 variants … prompt the immune system to produce antibodies that target viral regions the two strains have in common … XBB has evolved to elude antibodies induced by the vaccines and breakthrough infections.
Hence, the Nature study suggests, ‘current herd immunity and BA.5 vaccine boosters may not efficiently prevent the infection of Omicron convergent variants.'”
Indeed, a drawback of the original COVID shot that was widely ignored was that it only triggered the creation of antibodies against a single piece of the virus (the spike), whereas natural immunity creates antibodies against all of its parts.
Experts warned that embarking on a mass injection campaign would put enormous pressure on the spike that would result in mutations to evade immunity, and this is precisely what happened.
How Vaccines Can Drive Viruses to Mutate
The idea that vaccines can cause viral mutations is not new. As explained in “Vaccines Are Pushing Pathogens to Evolve,” published in Quanta Magazine14 in 2018, “Just as antibiotics breed resistance in bacteria, vaccines can incite changes that enable diseases to escape their control.”
The article details the history of the anti-Marek’s disease vaccine for chickens, first introduced in 1970. Today, we’re on the third version of this vaccine, as within a decade, it stops working. The reason for this is because the virus continuously mutates to evade the vaccine. What’s worse, the virus is also becoming increasingly deadly and more difficult to treat.
A 2015 paper15 in PLOS Biology tested the theory that vaccines are driving the mutation of the herpesvirus causing Marek’s disease in chickens. To do that, they vaccinated 100 chickens and kept 100 unvaccinated. All of the birds were then infected with varying strains of the virus. Some strains were more virulent and dangerous than others.
Over the course of the birds’ lives, the unvaccinated ones shed more of the least virulent strains into the environment, while the vaccinated ones shed more of the most virulent strains. As noted in the Quanta article:16
“The findings suggest that the Marek’s vaccine encourages more dangerous viruses to proliferate. This increased virulence might then give the viruses the means to overcome birds’ vaccine-primed immune responses and sicken vaccinated flocks.”
The take-home message here is that viruses mutate all the time, and if you have a leaky vaccine, meaning one that doesn’t block infection completely, then the virus will mutate to evade the immune response within that person.
As it happens, that is one of the distinct features of the COVID shots. They’re not designed to block infection. They allow infection to occur and at best lessen the symptoms, and as a result, the virus can mutate more or less unhindered. So, while the unjabbed were initially accused of being the ones responsible for mutations, it’s actually the jabbed who are the primary vectors.
Risk of COVID Infection Rises With Number of Shots
While newer variants can circumvent both “vaccine” immunity and natural immunity, natural immunity still provides far better protection, because the more shots a person gets, the more predisposed they become to COVID-19 infection.
This was most recently demonstrated in a Cleveland Clinic study,17 which concluded that the risk of COVID-19 infection “increased … with the number of vaccine doses previously received.” As reported by Finley:18
“Notably, workers who had received more doses were at higher risk of getting sick. Those who received three more doses were 3.4 times as likely to get infected as the unvaccinated, while those who received two were only 2.6 times as likely.
‘This is not the only study to find a possible association with more prior vaccine doses and higher risk of COVID-19,’ the authors noted. ‘We still have a lot to learn about protection from COVID-19 vaccination, and in addition to a vaccine’s effectiveness it is important to examine whether multiple vaccine doses given over time may not be having the beneficial effect that is generally assumed.'”
COVID Shots Suppress Your Immune Function
The COVID jabbed are also contracting other infections, as the shots weaken their innate immune system. In December 2022, MIT researcher Stephanie Seneff and Drs. Peter McCullough, Greg Nigh and Anthony Kyriakopoulos published a paper19 in which they described how the COVID shots inhibit the type-1 interferon pathway, which is the first-stage response to all viral infections.
As a result of this interferon inhibition, your innate immune system is suppressed, opening the door for all kinds of infections. Type-1 interferon also keeps latent viruses in check, so if your interferon pathway is suppressed, latent viruses, such as shingles, 20,21,22,23 can start to emerge. Importantly, cancer can also proliferate unchecked when your immune system is impaired.
Bivalent Boosters Are Minimally Effective at Best
The Cleveland Clinic study24 cited earlier also found that the bivalent COVID-19 booster was only 30% effective in preventing infection “during the time when the virus strains dominant in the community were represented in the vaccine.”
In other words, the boosters provide minimal protection even when well-matched to the circulating strain, and as its protection wanes, it leaves you at higher risk of infection than before.

Got the Jab? Take Action to Safeguard Your Health
If you already got one or more jabs and now have concerns about your health, what can you do? Well, first and foremost, never take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system.
If you developed symptoms you didn’t have before your shot, I would encourage you to seek out expert help. Unfortunately, most conventional doctors are clueless when it comes to COVID jab injuries (and vaccine injuries in general), so you’ll need to do some homework.
At present, the Front Line COVID-19 Critical Care Alliance (FLCCC) seems to have one of the best treatment protocols for post-jab injuries. It’s called I-RECOVER and can be downloaded from covid19criticalcare.com.25
Dr. Pierre Kory, who co-founded the FLCCC, has transitioned to treating the vaccine injured more or less exclusively. For more information, see DrPierreKory.com. Dr. Michelle Perro26 is also helping patients with post-jab injuries. I interviewed her about her treatment strategies in May 2022.
The World Health Council has also published lists of remedies that can help inhibit, neutralize and eliminate spike protein, which most experts agree is the primary culprit. I covered these in my 2021 article, “World Council for Health Reveals Spike Protein Detox.”
Other Helpful Treatments and Remedies
Other treatments and remedies that may be helpful for COVID jab injuries include:
•Hyperbaric oxygen therapy, especially in cases involving stroke, heart attack, autoimmune diseases and/or neurodegenerative disorders. To learn more, see “Hyperbaric Therapy — A Vastly Underused Treatment Modality.”
•Lower your Omega-6 intake. Linoleic acid is consumed in amounts 10 times higher than the ideal in well over 95% of the population and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. See “How Linoleic Acid Wrecks Your Health” for more information.
•Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. A dose of 15 to 80 milligrams a day could go a long way toward resolving some of the fatigue many suffer post-jab.
It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
•Near-infrared light, as it triggers production of melatonin in your mitochondria27 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,28 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
•Lumbrokinase and serrapeptidase are both fibrinolytic enzymes that, when taken on an empty stomach one hour before a meal, or two hours after, will help reduce your risk of blood clots.
- 1, 3, 5 CDC NCHS Data Brief December 2022
- 2 CDC Press release July 21, 2021
- 4 CDC Provisional Life Expectancy Estimates for 2021, August 2022
- 6 The Times October 10, 2020
- 7 Robert Malone Substack January 2, 2022
- 8 Our World in Data Excess Mortality During COVID Pandemic
- 9 KFF November 30, 2022
- 10 KFF Health System Tracker April 21, 2022
- 11 CDC Rates of COVID Cases or Deaths by Age Group and Vaccination Status
- 12, 18 WJS January 1, 2023
- 13 Nature December 19, 2022
- 14, 16 Quanta Magazine Vaccines Are Pushing Pathogens to Evolve
- 15 PLOS Biology July 27, 2015 DOI: 10.1371/journal.pbio.1002198
- 17, 24 MedRxiv December 19, 2022
- 19 Food Chem Toxicol June 2022; 164: 113008
- 20 Journal of Cutaneous Immunology and Allergy August 25, 2022
- 21 Rheumatology October 2021; 60(SI): 190-195
- 22 Channel 7 News April 20, 2021
- 23 J. Cosmet Dermatol November 2021; 20(11): 3350-3361
- 25 Covid19criticalcare.com
- 26 DrMichellePerro.com
- 27 Physiology February 5, 2020 DOI: 10.1152/physiol.00034.2019
- 28 Journal of Photochemistry and Photobiology February 2016; 155: 78-85





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr