Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- In mid-February 2023, I reported that the U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program
- Within days, fact checkers tried to debunk the idea that individual people are being tracked, or that these data could be misused by government or third parties
- COVID “vaccination” status was not considered a private medical matter at all during 2021 and 2022, yet mainstream media now want you to believe that your COVID jab status is protected by medical privacy laws
- Your medical data are not nearly as private as you think. The Health Insurance Portability and Accountability Act (HIPAA) is rife with exemptions when it comes to your privacy. Federal agencies such as Health and Human Services (HHS) and the Centers for Disease Control and Prevention, for example, are exempt from the privacy clauses and can access identifiable data — especially if there’s an outbreak of infectious disease, be it real or fictitious
- Government agencies and a number of third parties or “covered entities” can also use a number of loopholes to re-identify previously de-identified patient data
In mid-February 2023, I reported that the U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program designed by the U.S. National Center for Health Statistics (NCHS), a division of the Centers for Disease Control and Prevention.1
Within days, fact checkers were burning the midnight oil trying to debunk the idea that individual people are being tracked, or that these data could be misused by government or third parties.
Strangely enough, the most egregious “misinformation” example USA Today’s fact checker could find was a social media post that “generated nearly 200 likes in less than a month.”2 Two hundred likes? To most influencers, that’s nothing, especially not over the course of 30 days.
Why is USA Today stressing over a post with 200 likes? Seems a bit panicky if you ask me. Reuters also came out with a fact check and, like USA Today, Reuters claimed there was a lack of “context:”3
“New diagnostic codes that describe a patient as under-immunized against COVID-19 were introduced to help doctors identify patients potentially at risk for more-severe COVID and to help health officials track vaccine effectiveness and mortality statistics, among other public health questions, not for U.S. government tracking of unvaccinated individuals, as some are claiming online.
The codes in an individual’s medical record, like all personal health information, are protected by U.S. privacy law and could only be analyzed at the group or population level uncoupled from individual identities …”
Your Medical Records Are Far From Private
As is so often the case, the fact checkers are the ones taking the issue out of context or, rather, not presenting the full picture. The fact is, your medical data are not nearly as private as you think. The Health Insurance Portability and Accountability Act (HIPAA) is rife with exemptions when it comes to your privacy.
Federal agencies such as Health and Human Services (HHS) and the Centers for Disease Control and Prevention have every right to access identifiable information, as they are exempt from the privacy clauses, and they’re particularly justified to access your private vaccination data if there’s an outbreak of infectious disease, be it real or fictitious. As noted in the HHS’s and CDC’s HIPAA guidance:4
“Balancing the protection of individual health information with the need to protect public health, the Privacy Rule expressly permits disclosures without individual authorization to public health authorities authorized by law to collect or receive the information for the purpose of preventing or controlling disease, injury, or disability, including but not limited to public health surveillance, investigation, and intervention …
[T]he Privacy Rule expressly permits PHI [protected health information] to be shared for specified public health purposes. For example, covered entities may disclose PHI, without individual authorization, to a public health authority legally authorized to collect or receive the information for the purpose of preventing or controlling disease, injury, or disability …
Further, the Privacy Rule permits covered entities to make disclosures that are required by other laws, including laws that require disclosures for public health purposes.”
Loopholes Also Allow Re-Identification of Personal Data
Government agencies and a number of third parties or “covered entities” can also use a number of loopholes to re-identify previously de-identified patient data. As explained in a CDC Public Health Law document detailing the lawful sharing of private medical data:5
“While HIPAA limits the use and disclosure of health information, it also permits certain secondary use exceptions for public health purposes. HIPAA provides certain circumstances under which patient data can be disclosed to health departments without patient authorization.
Under HIPAA, providers may disclose identifiable patient data (protected health information or PHI) if required by law, allowing states to pass legal exceptions to HIPAA restrictions.
Providers may also disclose PHI to health departments without patient authorization for public health activities, such as communicable disease reporting, or to a public health authority to prevent or control disease, injury, or disability under the public health exemption. A covered entity may access, use, and disclose PHI for clinical research without an individual’s authorization if:
1)it obtains documentation of waiver of individual’s authorization by an institutional review board or privacy board
2)the PHI is necessary for this research
3)the research is using PHI of decedents
Providers may disclose EHI without patient authorization when the data have been ‘de-identified’ … but still permits re-identification by providers or regional health information organizations through randomized patient source codes should a public health alert or case report become necessary.
Finally, providers may disclose a ‘limited data set,’ including dates and zip codes, without authorization and still re-identify patients if they maintain patient codes derived from certain identifiers.”
So, can your vaccination status be accessed by federal health agencies? Yes. Can that information be identifiable? Absolutely yes. Does that mean that you, as an individual, could be surveilled and/or get caught in a forced vaccination dragnet or end up experiencing negative repercussions in other areas of your life due to your vaccination status? Probably.
U.S. “privacy” laws certainly make allowances for such scenarios, and considering the behavior of government over the past three years, it would be naïve to believe they would never use your vaccination data against you.

Download this Article Before it Disappears
Reuters Muddies the Water
Reuters also muddies the water in other ways. For example, the fact check stresses that medical providers have used the general code Z28.3 (which represents “underimmunized”) since 2015, and that “these codes are not used with purposes beyond monitoring and reporting diseases and mortality statistics or for insurance billing.”
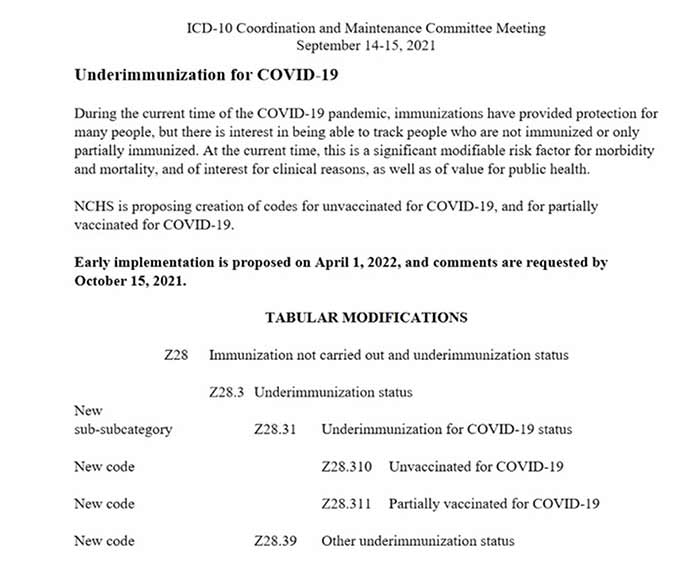
While it’s true that the International Classification of Diseases (ICD) code Z28.3 has been around for years, the new subcodes that track COVID jab status were added in mid-September 2021 during a ICD-10 Coordination and Maintenance Committee meeting, and during that meeting, they specified that “there is interest in being able to track people who are not immunized or only partially immunized.”
Below is a screenshot of page 194 of the agenda6 distributed during that meeting. There’s no ambiguity here. The new ICD-10 codes were added for the specific purpose of “tracking people” who are unjabbed or only partially jabbed against COVID-19.
They didn’t say they wanted to track “general population data.” They specifically said “people” are to be tracked. They also clearly state that this tracking is “of value for public health” — and again, the key words “public health” open the door to federal health agencies accessing identifiable data.
Moreover, additional subcodes specify the “why” a person chose not to get the COVID shot or stopped getting boosters. Those codes are listed in the screenshot below, under Z28.3 Underimmunization Status.7
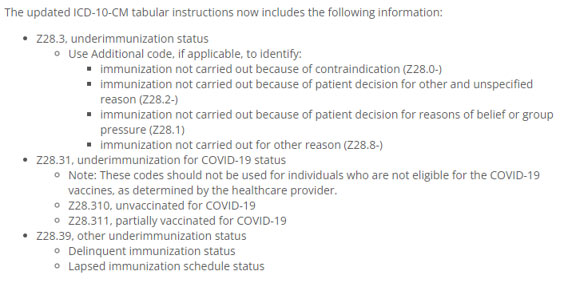
The use of “delinquent immunization status” under code Z28.39 also tells us something about where this is all headed. “Delinquent” means being “neglectful of a duty” or being “guilty of an offense.” Is refusing boosters a criminal offense? Perhaps not today, but some day, it might be, and these codes lay the foundation for that kind of medical persecution.
All Missed Vaccinations Will Be Tracked
Another tipoff that these codes will become part and parcel of the biosecurity control grid, even if they’re not used in this way now, is the fact that code Z28.39 — “Other underimmunization status”8 — is to be used “when a patient is not current on other, non-COVID vaccines.”9
In other words, they have already begun tracking ALL of your vaccinations, not just the COVID shot, and they can use the Z28.3 sub-codes to identify why you refused a given vaccine.
They’ve also added a billable ICD-10 code for “immunization safety counseling,” which explains the codes detailing “why” you refused a vaccine. So, if you didn’t get a vaccine due to “personal decision” (code Z28.2), or due to “personal beliefs or group pressure” (code Z28.1), then your doctor can bill your insurance for regurgitating vaccine propaganda and trying to change your mind.
Codes Could Be Put to Good Use
Giving credit where credit is due, Reuters Fact Check did point out a potentially beneficial purpose for the new ICD-10 codes:10
“[Eric Burnett, who specializes in hospital and internal medicine at Columbia University] said the ICD-10 codes could also help track data on vaccine efficacy, including comparisons between vaccination statuses of hospital or ICU patients with COVID, or patient mortality data based on vaccination status.”
That would be great, but the risk of these data being misused by the government is, I believe, greater than the possibility of them being used to protect the public from dangerous mRNA shots, seeing how overwhelming amounts of data showing harms are already being willfully ignored.
CDC Refuses to Answer Questions About the New Codes
Another red flag is the fact that the CDC has refused to answer questions about how it intends to use the new ICD-10 codes. In mid-February 2023, nine House Republicans sent a letter to the CDC demanding answers to these five questions:11
- Why did the CDC and National Center for Health Statistics (NCHS) decide to start gathering data on why Americans chose not to take the COVID-19 vaccine?
- How do the CDC and NCHS intend to use these new COVID-19 vaccination ICD codes?
- What steps are the CDC and NCHS taking to ensure that Americans’ private health information contained in the ICD system is protected?
- Will the CDC and NCHS confirm that they have not, will not, and cannot create a database of Americans based on their COVID-19 vaccination status?
- Can the CDC and NCHS confirm that private companies do not have access to lists of Americans’ COVID-19 vaccination status through the ICD system, or any other database overseen by the CDC and NCHS
As reported by The Daily Signal February 28, 2023, the CDC for some reason does not want to answer these questions:12
“The Centers for Disease Control and Prevention told The Daily Signal that it ‘will not be tracking’ the reasons Americans give for refusing to take a COVID-19 vaccine … Meanwhile, congressional Republicans told The Daily Signal that the CDC failed to respond to their questions by a deadline last week.
‘Two weeks ago, we sent a letter to the CDC demanding answers about its new COVID-19 vaccine database,’ Rep. Josh Brecheen, R-Okla., told The Daily Signal in a statement …
‘The CDC is stonewalling us and refusing to respond. Why won’t the CDC explain why it’s gathering data about Americans’ personal choices? House Republicans are not afraid to use the budgetary process to keep the CDC accountable to the American people,’ Brecheen warned.
House Republicans raised the alarm about the CDC’s involvement with the World Health Organization’s recently codified International Classification of Disease, or ICD, codes related to COVID-19 vaccination status, which went into effect last April. The codes enable the Centers for Disease Control and Prevention to collect data on the reasons Americans refuse to take one of the vaccines …
‘The ICD codes were implemented in April 2022, however the CDC/NCHS does not have any data on the codes and will not be tracking this information,’ Nick Spinelli, a CDC spokesman, said in an emailed statement. ‘The codes are developed and managed by the World Health Organization to enable healthcare providers to track within their practices …'”
End Goal Is Global Database for the Vaccine Passport System
The mention of the WHO brings me to my next point, which is that all of this information will likely, eventually, be transferred into a global vaccination database. Hence the reason why the WHO develops and manages the ICD-10 codes. It’s to allow for the “harmonization” of health care across the world.
Incidentally, the fact that the WHO develops and manages these codes also means that the WHO has approved these new codes that track vaccination status, and we already know that the WHO is working on a global vaccine passport.
To work properly, a global vaccine passport system needs a global vaccination database, and there’s no telling what privacy measures, if any, such a database might end up with. What we do know is that white papers13 and proposed legislation14 published during the COVID era that discuss health tracking and/or vaccine passports have stressed that privacy concerns must be relaxed or dropped altogether to ensure global biosecurity.
We also saw how COVID “vaccination” status was not considered a private medical matter at all during 2021 and 2022. In many places, you had to disclose your status and show proof that you’d been jabbed. Yet mainstream media now want you to believe that your COVID jab status is protected by medical privacy laws. What a joke.
As noted by Dr. Robert Malone in a January 25, 2023, Substack article, this vaccine passport system is being put into place right under our noses, and it would be incredibly naïve to think that these new ICD-10 codes are not part of that scheme:15
“The administrative state is busy building a vaccine passport system that will be active before most Americans are aware of what is being done to them. No one is going to knock on your door asking for your vaccine status because they already know …
They don’t need approval from Congress or the courts because we have given them the information through our health care providers. The CDC is the governmental organization tasked with tracking vaccine status on individuals.
They already have the records, as well as updated booster information. They just need to tweak a definition here and there, or get President Biden to keep the COVID-19 public health emergency in place indefinitely and the vaccine passports will be a fait accompli.”
A Data Collection Dragnet
As of January 1, 2014, the U.S. government required public and private health care providers to adopt and use electronic medical records (EMR) if they wanted to quality for full Medicaid and Medicare reimbursement.
The government also financially incentivized physicians and hospitals to adopt electronic HEALTH records or EHR.16 The difference between EMR and EHR is that EHR provides a far more comprehensive patient history than EMR, as it contains a patient’s medical history from more than one medical practice.
In essence, EHR is what you get when doctors share your medical data to create one comprehensive file that covers all your interactions with the medical system. While that sounds good in theory, Big Pharma immediately seized the opportunity to misuse it by placing drug ads within the EHR system.
This in turn has driven up medical costs and resulted in poor prescribing decisions that put patients at risk.17 Patients are also directly targeted with drug marketing through patient portals.
Physicians and hospitals who adopted EHR got paid extra. Between January 1, 2011 and December 31, 2016, the Centers for Medicare & Medicaid Services (CMS) paid out EHR incentive payments to hospitals totaling $14.6 billion.18 Meanwhile, those who chose not to capture, share and report clinical data on patients were financially penalized through reduced Medicare reimbursements.19,20
Needless to say, these “sticks” and “carrots” led to the rapid adoption of both EMR and EHR, both of which government requires if it wants the power to control the population through medicine, and we now know that’s exactly what government intends to do.
Transhumanism Is Being Implemented Through Food and Medicine
At the end of September 2022, President Biden laid out a “bold goal” to “end hunger and increase healthy eating and physical activity by 2030” through a federally-backed “Food Is Medicine” campaign.21
Integrating food and nutrition with health care so that food and health policies are under one umbrella will facilitate the creation of new policies, funding and control over both areas. Eventually, food purchases and health records will be linked to your vaccine passport/digital identity, which also holds your educational records, travel records, work records and bank accounts.
That this “Food Is Medicine” campaign has nothing to do with promoting real nutrition or whole food is obvious, as that same month Biden also signed the “Executive Order on Advancing Biotechnology and Biomanufacturing Innovation for a Sustainable, Safe and Secure American Bioeconomy.”22
This specifies that biotechnology and genetic engineering be used to transform the food and medical industries in order to promote a transhumanist agenda. It’s all about creating fake, synthetic and genetically manipulated foods and tinkering with the human genome.
On a larger scale, this plan is also promoted by the World Health Organization, which is trying to seize power over health care globally through International Health Regulation (IHR) amendments and the Pandemic Treaty. For more information on that, see “Pandemic Treaty Will Usher In Unelected One World Government.”
The WHO is also seeking to put food, medicine and climate under one umbrella. This would allow it to control the global population in any number of ways, as a climate issue could be positioned as a public health issue, or a food issue, and vice versa. In other words, people could be forced to eat bugs instead of beef because it “benefits the climate.” Private vehicle use could be restricted because it helps lower vehicular pollution that endangers public health, and so on.
So, to bring us full circle back to where we started, while media are now trying to lull you to sleep with “promises” that there’s nothing nefarious about tracking the unvaccinated or “undervaccinated,” think long and hard before you close your eyes to the possibility that this is all part of biosecurity-based totalitarian control grid.
- 1 PJ Media April 8, 2023
- 2 USA Today March 10, 2023
- 3, 10 Reuters February 21, 2023
- 4 CDC HIPAA Privacy Rule and Public Health
- 5 CDC Public Health Law
- 6 CDC ICD-10 Coordination and Maintenance Committee Meeting September 14-15, 2021
- 7 Naked Emperor Substack January 27, 2023
- 8 ICD10data Underimmunization
- 9 AAFP New Diagnosis Codes
- 11, 12 The Daily Signal February 28, 2023
- 13 The Rockefeller Foundation, National COVID-19 Testing Action Plan — Strategic Steps to Reopen Our Workplaces and Our Communities, April 21, 2020 (PDF)
- 14 Congress.gov HR 6666
- 15 RW Malone Substack January 25, 2023
- 16, 20 USF Health February 16, 2017, Updated March 4, 2023
- 17 AMA June 16, 2021
- 18 OIG HHS EHR Incentive Payments to Hospitals
- 19 AMA EHR Incentive Programs
- 21 Health.gov Conference on Hunger, Nutrition and Health
- 22 Executive Order on Advancing Biotechnology and Biomanufacturing Innovation for a Sustainable, Safe and Secure American Bioeconomy





")












Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr