Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- Since mRNA shots contain several novel technologies, they should be subject to more controls than conventional vaccines. Yet they aren’t. In fact, they’re not covered by any specific regulations
- mRNA COVID shots are gene therapy, but not regulated as such. By slapping a fraudulent “vaccine” label on gene therapies, they are being developed outside of the regulatory framework that governs them
- An alternative framework that could regulate mRNA shots would be Type1A pro-drug regulations, but they’re not being regulated as such either
- Per the U.S. Food and Drug Administration’s definition, gene therapy covers two modes of operation. It either alters the biological properties of living cells, and/or modifies your genes. This means that even if the product does not modify your genes, it’s still a gene therapy if it modifies the properties of cells, which is what the COVID shots do
- Data show 1 in 3 Pfizer COVID shots administered in Denmark were placebo — and regulators must have known about it
While the COVID-19 shots are referred to as “vaccines,” they do not meet the classical definition of a vaccine. Health authorities needed to change the definition1 to accommodate the COVID shots and shut down the argument that, as experimental gene therapies, they may be riskier than traditional vaccines.
Meanwhile, based on the U.S. Food and Drug Administration’s definition2,3 of “gene therapy” they’re clearly gene therapies, and both Moderna4 and BioNTech5 acknowledge this in their Securities and Exchange Commission (SEC) registration statements.
In a 2014 paper,6 BioNTech founder Ugur Sahin also stated that “One would expect the classification of an mRNA drug to be a biologic, gene therapy or somatic cell therapy.”
Publicly, however, drug makers, regulators and, of course, the media, have been going to great lengths to make sure people don’t think of them that way. Now, a peer-reviewed paper7,8 has weighed in on the controversy, stressing that mRNA COVID shots “should be labeled as gene therapy.”
mRNA Shots Are Gene Therapy, but Not Regulated as Such
As noted in this paper, published in the International Journal of Molecular Science, June 22, 2023:
“COVID-19 vaccines were developed and approved rapidly in response to the urgency created by the pandemic. No specific regulations existed at the time they were marketed. The regulatory agencies therefore adapted them as a matter of urgency.
Now that the pandemic emergency has passed, it is time to consider the safety issues associated with this rapid approval. The mode of action of COVID-19 mRNA vaccines should classify them as gene therapy products (GTPs), but they have been excluded by regulatory agencies.9
Some of the tests they have undergone as vaccines have produced non-compliant results in terms of purity, quality and batch homogeneity. The wide and persistent biodistribution of mRNAs and their protein products, incompletely studied due to their classification as vaccines, raises safety issues.
Post-marketing studies have shown that mRNA passes into breast milk and could have adverse effects on breast-fed babies. Long-term expression, integration into the genome, transmission to the germline, passage into sperm, embryo/fetal and perinatal toxicity, genotoxicity and tumorigenicity should be studied in light of the adverse events reported in pharmacovigilance databases.
The potential horizontal transmission (i.e., shedding) should also have been assessed. In-depth vaccinovigilance should be carried out. We would expect these controls to be required for future mRNA vaccines developed outside the context of a pandemic.”
mRNA Shots Do Not Qualify as Vaccines
Banoun goes on to review the definitions of vaccine and gene therapy as listed by the FDA, the European Medicines Agency (EMA), the World Health Organization and the French Agence Nationale de Sécurité du Médicament (ANSM). Of these, the ANSM and EMA specify that a vaccine must contain one or more antigens.
Based on that definition, mRNA shots do not qualify as vaccines in France and Europe, because they don’t contain antigens. The active substance that elicits a downstream immune response is mRNA. The mRNA instructs your cells to produce the antigen. The mRNA is not an antigen in and of itself. In the case of COVID-19, the antigen being produced downstream is a modified SARS-CoV-2 spike protein.
According to the U.S. Centers for Disease Control and Prevention’s updated definition,10 a vaccine is a preparation that stimulates an immune response against disease. The classical definition specified that a vaccine would result in immunity against the disease in question, but this specificity was removed to accommodate the COVID shots.11
Still, the mRNA injections clearly fall under the FDA’s definition of a gene therapy, because gene therapy:12
“… seeks to modify or manipulate the expression of a gene or to alter the biological properties of living cells for therapeutic use. Gene therapy is a technique that modifies a person’s genes to treat or cure disease …”
Note that gene therapy covers two different modes of operation. A gene therapy is something that either alters the biological properties of living cells, and/or modifies your genes. This means that even if the product does not modify your genes, it’s still a gene therapy if it modifies the properties of cells, which is precisely what the COVID shots do.

Download this Article Before it Disappears
mRNA Jabs Remain Outside of Regulatory Definitions
The author of that International Journal of Molecular Science paper, independent researcher Helene Banoun, compares the controls required by regulations for gene therapy products to those applied to the COVID shots, and the potential safety issues that arise due to the absence of these controls.
Importantly, Banoun points out that since mRNA COVID shots contain several novel technologies, they “should be subject to more controls than conventional vaccines.” Yet they aren’t. They’re not even covered by any specific regulations.
As noted in a May 2022 paper in Advanced Drug Delivery Reviews,13 “The current guidelines either do not apply, do not mention RNA therapeutics, or do not have widely accepted definition.” This, even though there are several highly relevant differences between conventional vaccines and mRNA therapeutics.
In other words, the mRNA shots are in a sort of limbo, from a regulatory point of view, still to this day. Health authorities are using them, promoting them and authorizing updated shots even though there’s no regulatory framework to ensure their safety.
mRNA Shots Being Rolled Out Without Regulatory Guidelines
Clearly, this cannot be allowed to continue, seeing how vaccine manufacturers are now replacing a long list of classic vaccines with mRNA-based ones. They’re also developing and testing so-called mRNA “vaccines” against noninfectious diseases such as cancer, and as noted by Banoun:14
“We must be very vigilant about the term vaccine associated with therapeutic drugs, particularly with regard to the regulations that apply to them. These therapeutics are not vaccines against infectious diseases and must therefore continue to comply with GTP [gene therapy product] regulations.”
In other words, by slapping a fraudulent “vaccine” label on gene therapies for noninfectious diseases, they can and are being developed outside of the regulatory framework that governs them. An alternative framework that could regulate mRNA shots would be Type1A pro-drug regulations, but they’re not being regulated as such either. As noted by Banoun:15
“According to the FDA, mRNA vaccines correspond to the TypeIA of pro-drugs,16 which are substances that are converted by cells into active drugs. This pro-drug property could imply additional controls to those applied to vaccines. However, neither the FDA nor the EMA make any reference to these qualifications for mRNA anti-COVID-19 vaccines.”
So, these shots are not being regulated as gene therapies, nor as pro-drugs, even though these are the only two definitions that correctly describe them. As research scientist Dr. David Wiseman explained in an interview with The Epoch Times:17
“With a conventional vaccine, you have the antigen, and you inject it into a person, and that is the thing that your immune system looks at and says, ‘ah ha,’ we need to make antibodies, T-cells, and other immune system components to what’s being injected.
The prime reaction of an mRNA vaccine is that it instructs the body how to make the antigen of interest. So, it’s similar to a pro-drug, which is converted inside the body via metabolism and enzymes into the desired drug effect.
The substance you’re injecting isn’t doing the final action; it leads to the thing that does the final action. With a pro-drug, the molecule you inject does not get changed into the final molecule of the antigen, it simply provides instructions because it’s gene therapy.”
Wiseman also noted that while the FDA can “change or exclude whatever they want from regulatory guidance … it doesn’t change the biologic definition of the product.” And, “since Pfizer and Moderna COVID-19 vaccines meet the definition of gene therapy, they should be handled according to gene therapy guidelines.”
COVID Jabs Bypassed Essential Studies
Because the COVID jabs were not classified as gene therapy, tests required for this drug class were not performed, including tests to assess:
| Genotoxicity | Genome integration |
| Germ-line transmission | Insertional mutagenesis |
| Tumorigenicity | Embryo, fetal and perinatal toxicity |
| Long-term expression | Biodistribution |
| Environmental excretion, such as shedding through seminal fluid, sweat or breast milk |
On top of that, the mRNA COVID shots also failed to meet basic standards required for vaccines, such as product purity standards. Investigations have revealed massive contamination issues, as well as wild variations in strength and purity of batches.
Commenting on the lack of testing performed on the COVID shots, Wiseman told The Epoch Times:18
“Several studies should have been done but weren’t done because they fell under the auspices of vaccines. But if you read the guidelines, it doesn’t say these studies are unnecessary, just that circumstances may deem them unnecessary.
We need laws for products that say you can’t just exclude them from regulations because you feel like it — because they are still gene therapies. We are hijacking the machines of our bodies to produce spike proteins in an uncontrolled, undefined way — there are too many things we don’t know about.”
Unregulated mRNA Shots Are a Pandora’s Box
Banoun writes:19
“The long-term safety monitoring of GTPs [gene therapy products] is required over several years whereas, for vaccines, it is generally only carried out over a few weeks. This should not be acceptable, given the persistence of the drug product and the expressed protein.
The known results of anti-cancer therapies and mRNA vaccines could lead us to anticipate problems of safety and efficacy. In the case of anti-cancer mRNAs, the vast majority of open-label clinical trials have been carried out on very small numbers of patients, with either unpublished or negative results.
Randomized studies also showed negative results, reporting more frequent adverse events in the treatment group. Concerning infectious diseases, two trials of mRNA vaccines encapsulated in LNPs [lipid nanoparticles] showed notable adverse effects.
A trial of an mRNA vaccine against rabies showed numerous adverse effects superior to those of the classic vaccine, which is already very reactogenic, notably lymphopenia (this effect was also found for anti-COVID-19 mRNA vaccines).
An influenza vaccine trial showed severe adverse effects in humans (31 subjects were observed over only 43 days and at least 4 serious adverse effects were found) … According to another HIV trial of 15 participants against a placebo, immune responses were unsatisfactory and of limited duration.
The founder of BioNTech himself, Ugur Sahin, warned20 against the use of codon optimization, which can alter translation speed and lead to misfolding. He also underlined the potential toxicity of unnatural nucleotides. He also mentioned the wide biodistribution of mRNA injected intramuscularly. He reminded us that we should fear the appearance of anti-self mRNA antibodies in patients suffering from autoimmune diseases …
The WHO declared an end to the emergency phase of the COVID-19 pandemic at the beginning of May 2023 but will continue to authorize the use of the Emergency Use Listed (EUL) procedure.
The emergency authorization of vaccines should be transformed into prequalification via a smooth transition. However, a wide-ranging public discussion should be opened on this transition to the routine use of mRNA vaccines, without them being subject to the controls required for GTPs.”
One-Third of Pfizer Shots Were Placebo
In related news, Kim Iversen recently broke the bombshell story that 1 in 3 Pfizer COVID shots administered in Denmark were placebo — and regulators must have known about it. The data for this claim comes from a Letter to the Editor published in the European Journal of Clinical Investigation at the end of March 2023.21
The three authors decided to investigate the potential for batch-dependent variations in side effects. To do that, they examined the rates of suspected adverse effects (SAEs) between different BNT162b2 batches administered in Denmark, which has a population of 5.8 million people, between December 27, 2020, and January 11, 2022. What they discovered was shocking. As explained by the authors:
“SAEs were counted on a batch level by linking individual SAEs to the batch label(s) of BNT162b dose(s) that the subject had received. The total number of SAEs associated with each batch was divided by the number of doses in the batch to obtain the rate of SAEs per 1,000 doses …
[H]eterogeneity in the relationship between the numbers of SAEs and doses per vaccine batch was assessed by log-transformation followed by non-hierarchical cluster analysis and general linear model (GLM) test for differences in SAE rates between batches …
A total of 10,793,766 doses were administered to 4,026,575 persons with the use of 52 different BNT162b2 vaccine batches (2340–814,320 doses per batch) and 43,496 SAEs were registered in 13,635 persons, equaling 3.19?±?0.03 (mean?±?SEM) SAEs per person …
Batch labels were incompletely registered or missing for 7.11% of SAEs, leaving 61,847 batch-identifiable SAEs for further analysis of which 14,509 (23.5%) were classified as severe SAEs and 579 (0.9%) were SAE-related deaths.
Unexpectedly, rates of SAEs per 1,000 doses varied considerably between vaccine batches with 2.32 (0.09–3.59) (median [interquartile range]) SAEs per 1,000 doses, and significant heterogeneity was observed in the relationship between numbers of SAEs per 1,000 doses and numbers of doses in the individual batches.
Three predominant trendlines were discerned, with noticeable lower SAE rates in larger vaccine batches and additional batch-dependent heterogeneity in the distribution of SAE seriousness between the batches representing the three trendlines.
Compared to the rates of all SAEs, serious SAEs and SAE-related deaths per 1,000 doses were much less frequent and numbers of these SAEs per 1,000 doses displayed considerably greater variability between batches, with lesser separation between the three trendlines.”
In the video above, Iversen shows the linear graphs referred to here, which makes it easier to comprehend the implications of these data. To summarize, the data showed that in the most hazardous batches (marked in blue), the side effect ratio was between 1 in 10 and 1 in 6. In moderately-hazardous batches (green), the side effect rate was about 1 in 400.
Strangely, some batches (yellow) had no side effects associated with them whatsoever. These batches accounted for about 30% of the total doses given that year. How could that be? The only time this happens is when you have a control group that is given as an inert placebo.
Regulator Didn’t Test Placebo Shots
The plot thickens from there, because data also reveal that Danish regulators must have known that certain batches were placebo. How? As explained by Iversen, regulators must perform routine testing of batches at various times, and when another group of researchers compared the findings above with the batches tested, they discovered that:22
- All of the most toxic batches underwent sample testing by regulators
- All but two of the moderately toxic batches were tested
- Only one of the placebo batches were tested
As noted by Iversen on her show:
“What are the chances that the group that had no side effects whatsoever, that looks like placebo, that looks like saline solution … that none of them were tested except one, when all of the others were tested? The regulators knew they didn’t need to test the saline solution. It would have been a waste of their time, so they didn’t … That’s what [it] looks like.”
Hazardous Batches Contained Fewer Doses
Another factor that suggests the public was being experimented on is the fact that the most hazardous batches had far fewer doses per batch compared to the moderately-hazardous batches and the placebo batches.
“They were experimenting on people. There’s no other way to slice it,” Iversen says. “The only other thing that’s possible is that they were covering up for the massive number of side effects … and the only way to mitigate it, to keep the public calm and to keep taking [the] injection, is to give a chunk of them a placebo … This is criminal.”
Early on, I and many others warned that everyone was in fact participating in an experimental study, not just those who signed up for the clinical trials. This evidence suggests that’s exactly what happened. Some got a placebo and others got the real McCoy, but not the same formulation.
And, while this investigation only included people in Denmark, it’s quite possible the same kind of multidose or multiformulation testing was taking place in other countries as well. HowBad.info,23 for example has also shown that some batches are associated with far higher rates of serious and lethal side effects than others, and that some batches appear completely harmless.
‘Inexorable Rise in Excess Mortality’
In closing, The Daily Sceptic24 recently reviewed data showing excess mortality is continuing to rise, post-rollout of the COVID jabs, with no sign of stopping:
“… core non-respiratory mortality (NRM) trends, which have been very stable over the last 10 years or so, can provide a useful yardstick to measure any kind of extraordinary change that might occur.
Since the vaccine rollout there have indeed been radical changes to this metric … Unfortunately there is still no evidence of any real slowdown of this alarming development.
Here is a chart which shows what has been happening with raw non-respiratory mortality data during the four COVID years. The years are each displayed with 13 data-points of four-weekly (monthly) aggregated figures.
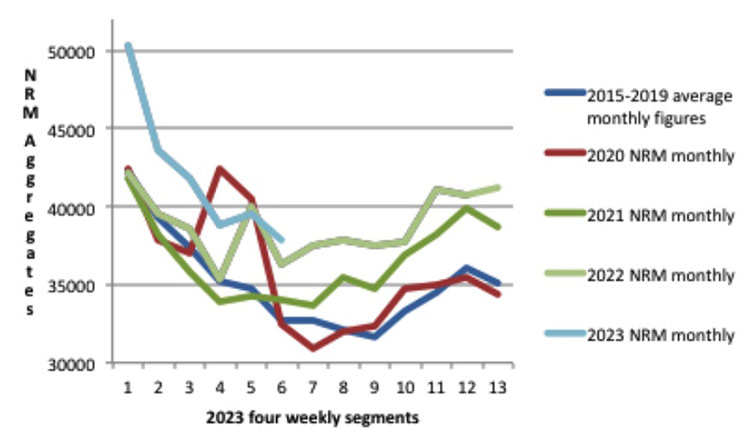
Each year appears to be worse than the previous one, and but for the still unexplained spike in non-respiratory deaths at the very beginning of the pandemic, 2020 would have been broadly similar to the 2015-2019 average. Something therefore happened in 2021 that changed the picture radically.
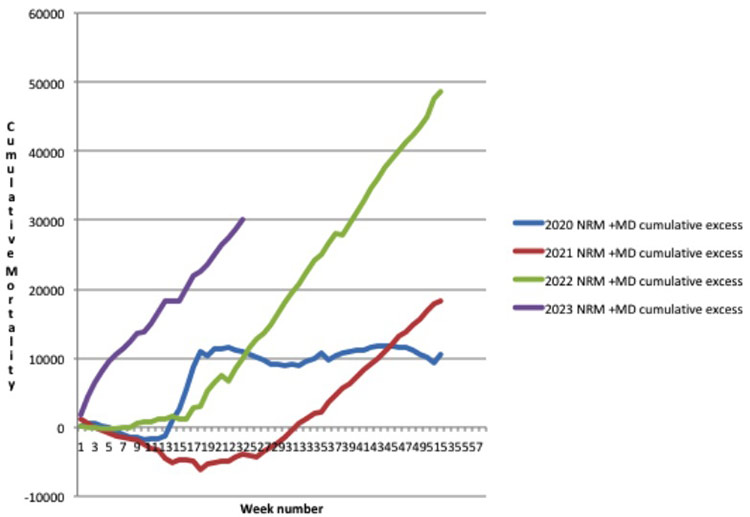
As all four COVID years are showing some excess non-respiratory deaths relative to the 2015-2019 average, the cumulative excess NRM can be displayed like this.”
Resources for Those Injured by the COVID Jab
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your body.
The same goes for anyone who has taken one or more COVID jabs and had the good fortune of not experiencing debilitating side effects. Your health may still be impacted long-term, so don’t take any more shots. If you’re lucky, perhaps you got saline, but I wouldn’t count on it. Besides, if you play Russian Roulette long enough, you’re bound to encounter a real bullet.
When it comes to treatment, it seems like many of the treatments that worked against severe COVID-19 infection also help ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
So, eliminating the spike protein your body is continuously producing is a primary task to prevent and/or address post-jab injuries. The two preferred remedies for this are hydroxychloroquine and ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein. Time-restricted eating (TRE) and/or sauna therapy can also help eliminate toxic proteins by stimulating autophagy.
The Front Line COVID-19 Critical Care Alliance (FLCCC) has developed a post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com25 (hyperlink to the correct page provided above). Additional detox remedies can be found in “World Council for Health Reveals Spike Protein Detox.”
- 1, 11 Pulse Substack November 9, 2021
- 2, 12 FDA Gene Therapy Definition
- 3 FDA Guidance for Industry January 2020
- 4 Moderna’s SEC Form S-1 Registration Statement
- 5 US SEC BioNTech 2019, Page 21
- 6 Nature Reviews Drug Discovery 2014; 13: 759-780
- 7, 14, 15, 19 International Journal of Molecular Science 2023; 24(13): 10514
- 8, 17, 18 The Epoch Times June 30, 2023
- 9 Frontiers in Medicine October 17, 2022; 9
- 10 CDC Immunizations: The Basics, Definition of Terms
- 13 Advanced Drug Delivery Reviews May 2022; 184: 114236
- 16 Pharmaceuticals October 14, 2009; 2(3): 77-81
- 20 Moderna. Quarterly Report Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the Quarterly Period […]. 6 August 2020
- 21 European Journal of Clinical Investigation Letter to the Editor March 30, 2023
- 22 Twitter Jessica Rose July 2, 2023
- 23 How Bad Is My Batch?
- 24 Daily Sceptic July 2, 2023
- 25 Covid19criticalcare.com





")










")
Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr