Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- According to a recent modeling experiment, “Increased contact among vaccinated people can give the false impression that COVID-19 vaccines are not working”
- This rationale is dubious at best, considering the unvaccinated have continuously been accused of not taking COVID seriously and going about their lives as normal, while the “vaccinated” are, by and large, more fearful and take “authorities” advice to heart, which includes avoiding large gatherings and close one-on-one interactions without wearing a face mask
- Many data sources reveal that COVID-jabbed individuals are now getting COVID-19 at far higher rates than the unjabbed. Death rates, both for COVID and other causes, have also risen in tandem with the number of shots administered
- According to an analysis of U.S. data, in September 2021, when Delta was most prominent, 23% of those who died from COVID had received the jab. In January and February 2022, when Omicron started dominating, that percentage jumped to 42%
- Many argue that Omicron was more contagious than Delta, hence the higher death toll. But Omicron was also far milder than Delta, and there’s no reason the jabbed would die at a higher rate from a less lethal variant than a more lethal one, unless the injection made the infection worse
- A preprint study found adult participants in Moderna’s trial who got the real injection and later got a breakthrough infection did not generate antibodies against the nucleocapsid — a key component of the virus — as frequently as did those in the placebo arm. Their anti-nucleocapsid response was also lower regardless of the viral load. As a result of this reduced antibody response, those who got the jab may be more prone to repeated COVID infections
Well, the COVID jab pushers have had to resort to all sorts of obfuscation to hide the fact that the injections don’t work, and now they’re really scraping the bottom of the barrel of excuses. According to a recent Reuters report,1 “Increased contact among vaccinated people can give the false impression that COVID-19 vaccines are not working.”
This irrational explanation has been levied in response to studies showing COVID-jabbed individuals are getting infected at higher rates than the unjabbed, and there are many such studies.
“These studies are likely to involve statistical errors, particularly if they did not account for different contact patterns among vaccinated versus unvaccinated people,” Korryn Bodner, a research associate in infectious disease modeling in Toronto, told Reuters. Bodner is the first author of a preprint study2 posted on medRxiv at the end of April 2022.
Are the Jabbed More Carefree Than the Unvaxxed?
Bodner’s claim is that those who got the jab may be more likely to throw caution to the wind and mingle with others, hence getting infected more frequently, while the unjabbed may be more cautious because they know they’re vulnerable. This rationale is dubious at best, considering:
a)The unvaccinated have continuously been accused of not taking COVID seriously and going about their lives as normal
b)Those who have taken the jab are, by and large, a far more fearful lot; they tend to listen to the “authorities” and take all of their advice to heart, which would include avoiding large gatherings and close one-on-one interactions without wearing a face mask
Check out the following story, reported by Anchorage Daily News:3
“Arianne Bennett recalled her husband, Scott Bennett, saying, ‘But I’m vaxxed. But I’m vaxxed,’ from the Washington hospital bed where he struggled to fight off COVID-19 this winter … Bennett went to get his booster in early December after returning to Washington from a lodge he owned in the Poconos, where he and his wife hunkered down for fall.
Just a few days after his shot, Bennett began experiencing COVID-19 symptoms, meaning he was probably exposed before the extra dose of immunity could kick in. His wife suspects he was infected at a dinner where he and his server were unmasked at times …
‘He was absolutely shocked. He did not expect to be sick. He really thought he was safe,’ Arianne Bennett recalled. ‘And I’m like, ‘But baby, you’ve got to wear the mask all the time. All the time. Up over your nose.'”
Within days of his third dose, he got a serious case of COVID. Yet they blame it on hypothetical exposure to an apparently healthy food server. This kind of irrational reasoning is prevalent among those who got the jabs and who keep going back for more as they are part of the 30% of the population that have been completely brainwashed.
To reiterate what I’ve explained since 2020, asymptomatic spread is likely to be so rare as to be nonexistent.4 It was a lie perpetuated to drive up fear and prop up rising “case” rates that didn’t really exist. It’s basic virology that you cannot transmit a virus unless you have a “hot” infection, and if you have an active, transmissible infection, you have symptoms. The symptoms are a sign that your body’s defenses are kicking in to rid itself of the live virus.
No symptoms, no transmission. So, unless the server was feeling sick and went to work anyway, the simplest explanation for Bennett’s demise was the shot itself. And if the server was sick, the fact that Bennett got so ill suggests the shot is ineffective, even at two doses.
The pro-pharma shills want you to believe there are so many confounding variables, we can’t possibly draw any conclusions from data showing the shots don’t work. Yet looking at data from a wide spectrum of sources, all show the same alarming trends. What “confounding factor” could possibly account for ALL of them being misinterpreted?
An Unproven Hypothesis
Reuters5 does note that Bodner’s simulations “do not prove that this type of bias affected studies of vaccine effectiveness versus the Omicron variant.” What it does show, according to Bodner, is that “even if vaccines work, increased contact among vaccinated persons can lead to the appearance of the vaccine not working.”
In other words, this is a hypothesis that has yet to be proven. Her modeling suggests it COULD make the jabs appear ineffective IF those who got the jab actually behave very differently from the unjabbed.
But again, it’s highly unlikely that the unvaccinated are avoiding exposure by steering clear of close contacts and crowds to a greater degree than those who got the jab. It’s far more reasonable to suspect that the shots don’t work.
On a side note, Bodner’s study was funded by the Canada COVID-19 Immunity Task Force.6 This task force is housed at McGill University in Montreal, Canada, and McGill University is a long-term recipient of grants from the Bill & Melinda Gates Foundation.7,8,9,10
What Do the Data Say About COVID Jab Effectiveness?
Based on data from around the world, it seems clear that the COVID gene transfer injections are not working. In fact, they’re having the opposite effect of what you’d expect from a real vaccine. According to a Washington Post analysis of state and federal data,11 in September 2021, when Delta was most prominent, 23% of those who died from COVID in the U.S. had received the jab.
In January and February 2022, when Omicron started dominating, that percentage jumped to 42%. In December 2021 and January 2022, just under half of all the COVID patients in intensive care at Kaiser Permanente’s hospital system in Northern California had also received one or more shots.12
Many argue that Omicron was more contagious than Delta, hence the higher death toll. But Omicron was also far milder than Delta, so why would the jabbed die at a higher rate from a less lethal variant than a more lethal one?
One attempt at an explanation is that the fatalities are now occurring primarily among the elderly. Nearly two-thirds of those who died from COVID during the Omicron wave were 75 and older. During the Delta wave, 75-year-olds and older accounted for just one-third of the deaths.13
But that was the case from the beginning, and it still doesn’t answer the question: Why would old people be more likely to die from a milder virus than a more serious one? To answer that question, the injection pushers revert back to the argument of waning potency. Two-thirds of those who died in January and February 2022 did not have a booster shot. According to Anchorage Daily News:14
“Experts say the rising number of vaccinated people dying should not cause panic in those who got shots, the vast majority of whom will survive infections. Instead, they say, these deaths serve as a reminder that vaccines are not foolproof and that those in high-risk groups should consider getting boosted and taking extra precautions during surges.”
So, in other words, the jab only works for a handful of months, and then you have to take another. And another. And another. According to the U.S. Centers for Disease Control and Prevention,15 the first two doses wear off after five months, necessitating a third dose, and the third dose wears off in just four months, at which time you’re supposed to get dose No. 4.
Israeli data16 show the effectiveness of shot No. 4 in preventing severe disease declines by 56% in just seven weeks. So, it appears the protection you get from the shots keeps getting shorter with each dose. Meanwhile, data show the shots can render you increasingly susceptible to all manner of infection and disease, through a wide variety of mechanisms.
Moderna Trial Data Reveal Repeated Infections Are Likely
Among such data is a preprint study17 posted on medRxiv April 19, 2022, which found adult participants in Moderna’s COVID jab trial who got the real injection, and later got a breakthrough infection, did not generate antibodies against the nucleocapsid — a key component of the virus — as frequently as did those in the placebo arm.
Curiously, placebo recipients produced anti-nucleocapsid antibodies twice as often as those who got the Moderna shot, and their anti-nucleocapsid response was larger regardless of the viral load. As a result of this reduced antibody response, those who got the jab may be more prone to repeated COVID infections. As reported by The Defender:18
“[T]he authors found that using the presence of anti-nucleocapsid (anti-N) antibodies to determine whether a person was exposed to SARS-CoV-2 will miss some infections. Thus, the sensitivity of this kind of test, when applied to vaccinated individuals, is not ideal.
However, there are more important implications19,20 of these findings … Specifically, the study implies that the reduced ability of a vaccinated individual to produce antibodies to other portions of the virus may lead to a greater risk of future infections in the vaccinated compared to the unvaccinated.
It is important to note that this is not just another argument for the superiority of natural immunity. Rather, this is evidence suggesting that even after a vaccinated person has a breakthrough infection, that individual still does not acquire the same level of protection against subsequent exposures that an unvaccinated person acquires.
This is a troubling finding, and something investigators conducting the Moderna vaccine trial likely knew in 2020.”
UK Data Confirm Results
These findings are corroborated by data from the U.K. Health Security Agency. It publishes weekly COVID-19 vaccine surveillance data, including anti-nucleocapsid antibody levels. The report21 for Week 13, issued March 31, 2022, shows that COVID-jabbed individuals with breakthrough infections have lower levels of these antibodies — a finding they attributed to the protective benefit of the shot:
“These lower anti N responses in individuals with breakthrough infections (post-vaccination) compared to primary infections likely reflect the shorter and milder infections in these patients.”
However, this interpretation is likely flawed, because less severe infection is associated with lower viral load, and as the study above demonstrated, the “vaccinated” have lower anti-nucleocapsid antibody levels than the unvaccinated at all viral load levels, but especially so at the lowest viral loads. As noted by The Defender:22
“This is one of the most significant findings of the study because it overturns the heretofore unchallenged idea that decreased seroconversion in the vaccinated is due to less severe infection in this population — which is a benefit provided by the vaccine.
However, this new study shows that even at low viral loads, the unvaccinated are more likely to seroconvert than those who are vaccinated. In fact, the difference in seroconversion rates is the greatest at lowest viral loads. The decrease in conversion rates is not a result of a benefit from the vaccine. It is a consequence of it.”
Boosted Now Have Three to Four Times Higher Case Rates
The Defender also reviews other U.K. data showing the COVID case rate is three to four times higher among those who have received a booster shot, compared to the unvaccinated. This is true for all age groups with the exception of children under 18:23
“What could explain such a large increase in infection rates among the boosted? Interestingly, the authors … warn that the unvaccinated may have contracted COVID-19 prior to the observation period — in other words, they may have acquired natural immunity previously, giving them added protection …
But their own data tells the opposite story. The boosted are more likely to contract the disease — by a factor of 3 to 4. How do we know whether the larger infection rates in the boosted are due to more robust immunity in the unvaccinated because of prior infection or due to an immune deficiency in the boosted?
The question can be definitively answered by examining the trend of infection rates [using] … the equivalent table from two months earlier. There is still a greater infection rate among the boosted, but it is only two to three times higher. If the authors’ hypothesis was correct, the more recent data should have shown less of a difference, not more.
If anything, their data support the finding that the decreased seroconversion rates in the vaccinated may be causing a greater risk of repeated infections.”
Walgreens’ Data
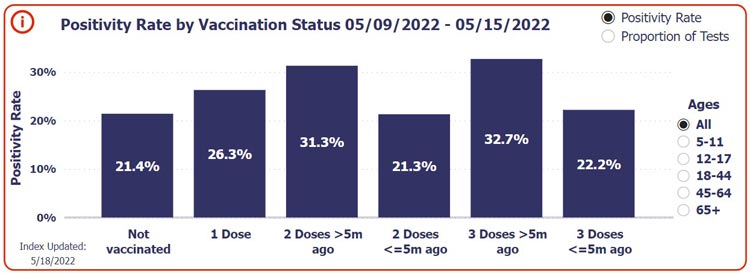
Data from the pharmacy chain Walgreens in the U.S. also reveal the same trend — COVID-jabbed individuals are testing positive for COVID at higher rates than the unjabbed, and those who got their last shot five months or more ago have the highest risk.
As you can see in the screenshot from Walgreens’ COVID-19 tracker24 below, during the week of May 9 through 15, 2022, 21.4% of unvaccinated individuals who got tested for COVID got a positive result. Of those who had gotten just one COVID shot, the positivity rate was 26.3%.
Of those who received two doses five months or more ago, 31.3% tested positive, and of those who received a third dose five months or more ago, the positive rate was 32.7%. So, after the first booster shot (the third dose), people are at greatest risk of testing positive for COVID.
More Jabs, More COVID Deaths

Perhaps most disturbing of all are the data showing the COVID shots are raising mortality rates, both from COVID and other causes. Above is an animated illustration25 sourced from Our World In Data, first showing the vaccination rates of South America, North America, Europe and Africa, from mid-December 2020 through the third week of April 2022, followed by the cumulative confirmed COVID deaths per million in those countries during that same timeframe.
Africa has had a consistently low vaccination rate throughout, while North America, Europe and South America all have had rapidly rising vaccination rates. Africa has also had a consistently low COVID mortality rate, although a slight rise began around September 2021. Still, it’s nowhere near the COVID death rates of North America, South America and Europe, all of which saw dramatic increases.
Here’s another one,26 also sourced from Our World In Data, first showing the excess death rate in the U.S. (the cumulative number of deaths from all causes compared to projections based on previous years), between January 26, 2020, and January 30, 2022, followed by an illustration of the tandem rise of vaccine doses administered and the excess mortality rate. It clearly shows that as vaccination rates rose, so did excess mortality.

Risk-Benefit Analyses
We also have the benefit of more than one risk-benefit analysis, and all show that, with very few exceptions, the COVID jabs do more harm than good. A risk-benefit analysis27 by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp, published in mid-February 2022, concluded that the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80.
Another analysis,28 which relied on data in the U.S. Vaccine Adverse Events Reporting System (VAERS), concluded that in those under age 18, the shots only increase the risk of death from COVID, and there’s no point at which the shot can prevent a single COVID death, no matter how many are vaccinated.
If you’re under 18, you’re a shocking 51 times more likely to die from the jab than you are to die from COVID if not vaccinated. In the 18 to 29 age range, the shot will kill 16 for every person it saves from dying from COVID, and in the 30 to 39 age range, the expected number of vaccine fatalities to prevent a single COVID death is 15. Only when you get into the 60 and older categories do the risks between the jab and COVID infection even out.
A third risk-benefit analysis by researchers in Germany and The Netherlands was published in June 2021, in the journal Vaccines.29 The paper caused such an uproar, part of the editorial board resigned in protest.30 The journal retracted the paper, but after a thorough re-review, it was republished in the August 2021 issue of Science, Public Health Policy and the Law.31
These researchers concluded that, “as we vaccinate 100 000 persons, we might save five lives but risk two to four deaths.”32 A fourth, still preliminary, analysis — based on more than 1,700 death reports collected by Steve Kirsch — shows the shots do more harm than good in anyone under age 60. Kirsch writes:33
“Figure 1 below is an analysis of survey data I collected. The analysis shows that the vaccines are harmful to those under 60. The red dots higher than the error bar means more vaccinated people observed dead than expected based on the population of vaccinated to all people.
In other words, if we vaccinated 60% of people (middle of the grey bar) and 70% (red dot) of the deaths are vaccinated, we have a serious problem. The precautionary principle of medicine suggests if you are under 60 and thinking of taking a vaccine, you shouldn’t. These preliminary results are both statistically significant …
The conclusion is very clear: nobody under 60 years old should get the vaccine because there is no evidence of a benefit. In fact, if you are between 40-60, it’s clear that vaccination makes it more likely you’ll die, not less likely.”
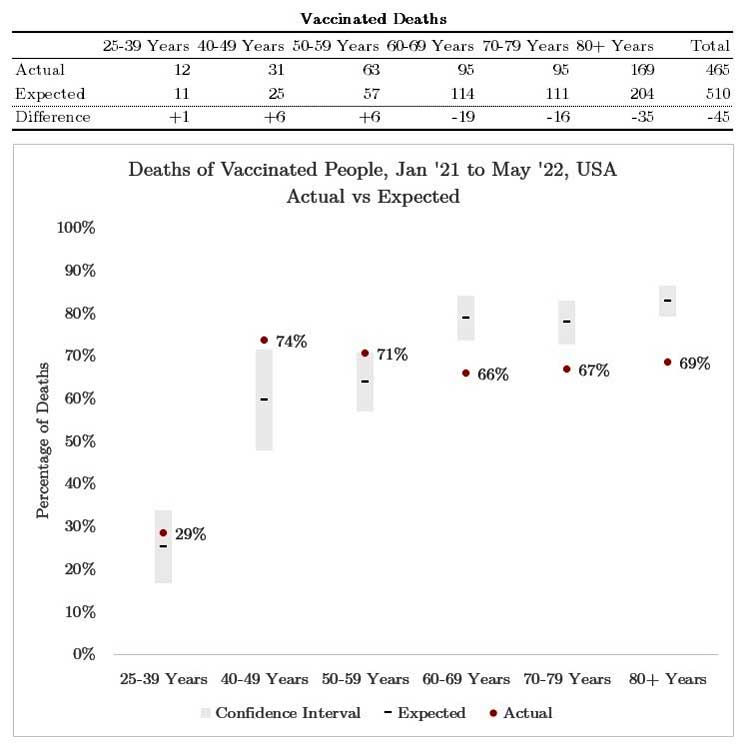 Figure 1. Red dot below error bar = vax works. Red dot above error bar = vax likely causes harm. Red dot inside the error bar = Insufficient evidence to justify taking a new, unproven vaccine. Conclusion: Vaccine shouldn’t be considered unless there is a clear benefit. 60 and older seems to justify use based on the data we have so far. Limitations: we are waiting for others to confirm / challenge the analysis. See text34 for more info. Joel Smalley did the analysis.
Figure 1. Red dot below error bar = vax works. Red dot above error bar = vax likely causes harm. Red dot inside the error bar = Insufficient evidence to justify taking a new, unproven vaccine. Conclusion: Vaccine shouldn’t be considered unless there is a clear benefit. 60 and older seems to justify use based on the data we have so far. Limitations: we are waiting for others to confirm / challenge the analysis. See text34 for more info. Joel Smalley did the analysis.While some analyses present a direr picture than others, taken together, it’s clear that there appears to be no long term benefits to the COVID jabs. We’re consistently ending up with a higher cost than can conceivably be considered reasonable. The pro-pharma side will likely continue to lob flimsy excuses at the data, but at some point, the truth will be so clear that even the blind will see it. Until that day, continue to inform yourself and share what you find.
- 1, 5 Medscape May 13, 2022
- 2 medRxiv April 29, 2022 DOI: 10.1101/2022.04.25.22274266
- 3, 11, 12, 13, 14 Anchorage Daily News April 29, 2022
- 4 Nature Communications November 20, 2020; 11 Article number 5917
- 6 medRxiv April 29, 2022 DOI: 10.1101/2022.04.25.22274266, See funding statement
- 7 Gates Foundation Grant to McGill University September 2020
- 8 Gates Foundation Grant to McGill University April 2020
- 9 McGill International Funding Sources
- 10 McGill newsroom December 17, 2015
- 15 CDC COVID-19 Vaccine Booster Shots
- 16 The Defender April 7, 2022
- 17 medRxiv April 19, 2022 DOI: 10.1101/2022.04.18.22271936
- 18, 22, 23 The Defender May 4, 2022
- 19 Igor’s Newsletter April 26, 2022
- 20 Bad Cattitude Substack April 27, 2022
- 21 UK Health Security Agency COVID-19 Vaccine Surveillance Report Week 13
- 24 Walgreens COVID-19 Index
- 25 Twitter TexasLindsay April 23, 2022
- 26 Twitter TexasLindsay April 25, 2022
- 27 COVID-19 and All-Cause Mortality Data Analysis by Kathy Dopp and Stephanie Seneff (PDF)
- 28 COVID Vaccination and Age-Stratified All-Cause Mortality Risk (PDF)
- 29 Vaccines 2021; 9(7): 693
- 30 Science, Public Health Policy and the Law August 2021; 3: 81-86, page 82
- 31 Science, Public Health Policy and the Law August 2021; 3: 87-89
- 32 Clinical and Translational Discovery February 25, 2022; 2(1): e35
- 33, 34 Steve Kirsch Substack May 17, 2022





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr