Analysis by Tessa Lena
STORY AT-A-GLANCE
- In October 2021, Dr. Spiro Pantazatos at Columbia University co-authored a paper (preprint) on risks associated with COVID injections
- His paper showed a statistically significant correlation between vaccination and all-cause mortality during the following month
- In the meanwhile, the university announced the mandates and invested into a digital system to enforce it
- Dr. Pantazatos wrote an extensive, thoroughly sourced letter demonstrating the lack of scientific foundation behind mandates for college students
- As a public service, he created a generic version of the document and made it publicly available so that other people can use it at their universities
This story is about one brave Columbia University researcher’s plight to defeat the mandates. The researcher in question is Spiro Pantazatos, Ph.D. He is an Assistant Professor of Clinical Neurobiology (Psychiatry) at Columbia University and a Research Scientist at the New York State Psychiatric Institute.
In October 2021, he co-authored a paper on risks associated with COVID vaccination (“vaccine-induced fatality rate” or “vaccine mortality risk”). I first wrote about his findings in April 2022, and then recently, I interviewed him about his latest important initiative, which is the reason for this article.
Dr. Pantazatos’ Paper on Vaccine Mortality Risk
The title of the paper, a preprint, is “COVID vaccination and age-stratified all-cause mortality risk.” According to Dr. Pantazatos’ findings, there was a statistically significant correlation between vaccination rates and all-cause mortality during the following month. From the paper:
“Accurate estimates of COVID vaccine-induced severe adverse event and death rates are critical for risk-benefit ratio analyses of vaccination and boosters against SARS-CoV-2 coronavirus in different age groups. However, existing surveillance studies are not designed to reliably estimate life-threatening event or vaccine-induced fatality rates (VFR).
Here, regional variation in vaccination rates was used to predict all-cause mortality and non-COVID deaths in subsequent time periods using two independent, publicly available datasets from the US and Europe (month-and week-level resolutions, respectively).”
The paper was inspired by Dr. Pantazatos’ co-author, Herve Seligmann, who analyzed European data that “showed a consistent trend where a vaccination campaign seemed to be accompanied by an increase in all-cause mortality during the month following the vaccination campaign.”
When Dr. Pantazatos saw the analysis of the European data, he “decided to do his own analysis based on the U.S. data (vaccinations and all-cause mortality), published by the CDC. And when he did his analysis using the U.S. data, it showed the same trend. His analysis of the CDC data showed that following a vaccination campaign in a given locality, there was an increase in all-cause mortality during the following month, followed by a decrease.”
And important factor that compelled Dr. Pantazatos to look into the data was the fact that his university was implementing the mandates, which struck him as unusual, assuming the injections really were as safe and effective as advertised.
Given today’s uninspiring intellectual environment in mainstream medical science and the atmosphere of censorship and self-censorship, there are very few brave souls among journal editors willing to publish his findings.
Early on, the paper was getting flat out rejected without even being sent out for peer review. Since then, things have gotten better, and there is some hope that it will get published, although the pushback is still very strong. Such is life of an honest scientist in a world that is led by uncurious people in power and almost entirely sponsored by Pfizer! But the thing about the truth is that is it, well, true, and so it has to eventually prevail, whatever it takes!
The Soul Journey
What’s immediately noticeable about Dr. Pantazatos is his grace and his impeccable mainstream presentation of the data. A few months ago, when I first watched an interview with him, I rejoiced over finally finding something that I could easily sent to my “respectable” friends and have them listen.
There is nothing sensationalist in Dr. Pantazatos’ presentation, nothing that can stylistically turn off a proud New York Times reader — and as he highlights the alarming statistical data regarding the injections, he does so with grace and with love for his less skeptical peers.
In his own life, when it all just started, he was not dissenting. He saw zero reasons for dissent, and he trusted the official message. Early on, like so many, he was very scared of COVID, and he planned to stay home until the vaccines came out. In fact, Dr. Pantazatos had very high hopes for those vaccines, and was awaiting them with great anticipation.
In the end, it was the data — telling a different story than the state bureaucrats and the media — that made him change his mind about the COVID injections. Vivat the scientific method!
Digital Passports?
During the interview, I asked Dr. Pantazatos about his thoughts on the reasons for the administration’s seeming unconditional love of the injections — and one of the things he mentioned as a possible factor was that the university had invested into creating a digital system that would only allow campus access to those who are fully up-to-date on the injections. (You can find Columbia University vaccination requirements here.)
In that light, it is possible that the school administrators are so financially and emotionally married to their status under the “new normal” that their otherwise capable minds are refusing to see the real-life data because the data would undermine their belief system. Most horrible things on Earth happen because good people accept them …
Furthermore, Dr. Pantazatos noted that, due to peer pressure, those experiencing possible side effects from the injections may find themselves in denial and look for explanations anywhere but the injection.
Dr. Pantazatos’ Letter to Columbia University
Dr. Pantazatos’ work for Columbia University is fully remote. None the less, he was told that in order to keep his job, he needed to comply with the mandates — and currently, he is in the process of submitting his exemption (let us pray for his success!)
In meanwhile, he created a very extensive, thoroughly sourced document that he sent to the President of the Columbia University to demonstrate the lack of scientific foundation behind the COVID injection mandates.
As a public service, Dr. Pantazatos created a version of the letter that can be used by others, and he made it publicly available. This initiative is in collaboration with attorney Kevin M. Barry from Mermigis Law Group. The recommendation is to take the template, make the necessary changes (the instructions in the document make it easy), sign it, print it out, and send it via certified mail, which might come in handy in case there is mandate-related legal action in the future.
The live version of the document (the main text of the letter, as well as all other sections and all references) can be found here. It is important to look at the live version as it may get updated with more data, more signatures, etc. The live version also has instructions. If you would like to download the current full version of the letter as a PDF, it can be found here.
The main section of the letter with respective refences is included below (please note that the full version contains additional sections, and that the numbers in square brackets refer to references at the end of the full document):
Dear President,
My name is Spiro P. Pantazatos, Ph.D. I am an Assistant Professor in clinical neurobiology and biomedical data science at Columbia University Irving Medical Center. I, along with several colleagues, write to you today to share a letter we sent to leadership at Columbia University in New York. We hope you will consider the data presented herein when deciding vaccine policies for your students.
As background, in December 2021, I contacted the Columbia University COVID response Director to share vaccine safety research and global policy updates, including Moderna vaccine restrictions for young adult males in Nordic countries due to safety concerns [1,2], and to notify the university of my presentation at the Columbia COVID Symposium on age-stratified risk-benefit analysis using data-driven vaccine mortality risk estimates from publicly available US CDC data1 [3].
To date, however, Columbia University still has not updated its COVID vaccine policies and guidelines. Hence, I prepared and recently sent my institution this letter which includes over 100 references and footnotes on why their policies and guidelines should be revised ASAP.
We request that your university update its vaccine policies and recommendations to reflect the most recent global data on the COVID vaccine and booster’s (limited) effectiveness, especially in relation to their increasingly apparent and concerning safety signals such as unacceptably high rates of myocarditis in young adult males [4–6].
This letter serves to notify your university of potential liability for proceeding with the current COVID-19 vaccination policy, which is based on the unfounded assumption that vaccines and boosters are sufficiently safe, necessary and effective in implementing its COVID-19 vaccine policies, especially for students who are mostly 24 years old or younger, which could potentially put your university’s endowment at risk.
Please see the references in this letter so the university can verify whether or not the university should rely on recommendations from public health agencies.
Please be advised that your university’s COVID vaccine policy makers should not blindly trust the FDA and CDC claims regarding the risk-benefit of COVID-19 vaccines when making decisions on University-wide vaccine policy.
Despite promising full transparency regarding the COVID-19 vaccines,2 the FDA had to be sued by NYC-based law firm Siri & Glimstad in September, 2021 just to release the Pfizer safety data they relied upon to issue the EUA and approval of the Pfizer vaccine (documents which should have been in the public domain to begin with).3 Moreover, the FDA requested the federal judge give them 75 years to release them.4
Fortunately, the judge denied the FDA’s request and ordered them to promptly release the documents. The first set of documents, released in March, 2022, show that 42,086 adverse events (AEs), including 1,223 deaths, 932 hematological, 1,403 cardiovascular, and 1050 autoimmune events were reported in the first 3 months of the Pfizer vaccine rollout.5
These events occurred within a median of 1 day or < 24 hours, evidencing a causal link to the vaccine. However, the Pfizer vaccine (marketed as Comirnaty) fact sheets for healthcare providers and patients do not mention any of these severe AEs other than myocarditis.6
Moreover, neither the fact sheets nor the CDC links cited in the fact sheets7 mention incidence rates for myopericarditis, and simply claim vaccine benefits outweigh the risks without providing any supporting data.
As of June 29th, 2022, the CDC indicates that 15,312 US deaths following COVID-19 vaccination have been reported to the Vaccine Adverse Events Reporting System (VAERS). While the fraction of deaths having an established causal association with vaccination has not yet been published, the CDC has used VAERS to report a crude mortality rate 0.0026%.8
This risk is higher than the risk of death following infection with omicron in young adults. In response to recent FOIA requests, the CDC has admitted they did not follow their own standard procedures for monitoring ‘early warning safety signals’,9 and apparently did not even begin looking at those signals until April 2021, 4 months after the vaccination program began.10
In January, 2022 the CDC director admitted vaccines cannot prevent transmission of currently circulating variants.11 There is therefore no justification to mandate or recommend vaccines or boosters to University undergraduate and graduate students, or any University staff or faculty member who does not wish to take them.
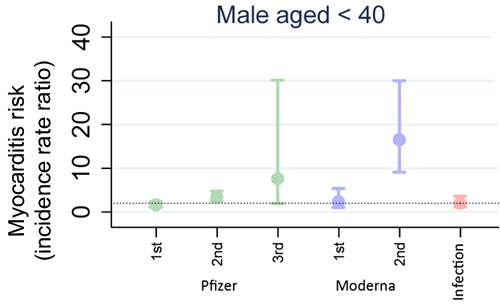
The cure may be worse than the disease. In males <40 years old, myocarditis risk following Pfizer 2nd and 3rd (booster) and Moderna 2nd dose is higher than myocarditis risk following SARS-CoV-2 infection, and the risk increases with each dose. Figure adapted from Patone et al.
Risk of myocarditis following sequential COVID-19 vaccinations by age which analyzed >40M health records from the English National Immunisation (NIMS) Database of COVID-19 vaccination. Graph plots myocarditis incident rate ratios relative to background rates. Dotted line shows risk following infection for visualization purposes.
The Hippocratic Oath says “First, do no harm”. On the basis of the above facts alone, the University-wide COVID-19 vaccine mandates should be lifted immediately and guidelines and recommendations adjusted accordingly in order to provide fully informed consent regarding vaccine and booster risks.
The rest of this letter elaborates and provides supporting data on the following four points (the references below mention Columbia University (CU) but are generally applicable):
A.Vaccine risks outweigh the benefits in most age groups, and particularly in adolescents and young adults where the infection mortality risk is extremely low (i.e. 0.003% and 0.006% in ages 15-19 and 20-24 respectively [7] who are the majority age group facing the mandates), and the vaccine risks appear to increase with each dose or booster.
B.Vaccines do not measurably reduce transmission and community spread. The originally stated purpose of most University vaccine mandate policies (i.e. to prevent COVID transmission and community spread) is not (and never was) backed by empirical evidence.
C.Vaccination is both unnecessary, and more risky, in individuals with previous coronavirus infection. Most university policies ignore the substantial body of evidence documenting robust and durable natural immunity and increased risks of vaccine adverse reactions in those with previous infection.
As of February 2022, about 75% and 67% of adolescents 12-17 and adults ages 18-49 respectively had infection-derived immunity and these proportions are likely higher today [8].
D.Publications and sources that claim or imply sufficient vaccine safety and favorable risk-benefits profiles are untrustworthy and unreliable because their raw data are inaccessible or their claims are not backed by supporting data or contradict existing evidence, especially for the student age population.
In light of the evidence presented herein, we urge the following actions and remediations be taken ASAP following receipt of this letter:
1.The vaccine and booster mandates should be lifted immediately, and any official University guidance and recommendations should be updated to provide true informed consent about vaccine safety risks. This includes removing vaccine requirements regarding access to campus and updating the University website which may contain misinformation about the safety, effectiveness and risk-benefit of the COVID vaccines, as necessary.
It causes more harm to mandate primary series vaccinations against variants that are no longer in circulation [9] and boosters that carry much higher risks relative to low-lethality omicron variants.
2.Replace any policy making bodies which mandated COVID vaccines (such as the Task Force at Columbia)12 with a more robust and inclusive method for deciding future University-wide health policy decisions. Columbia University’s leadership and COVID task force failed to conduct reasonable due diligence to ensure the safety and health of the Columbia community.
Perhaps your University had a similar policy making body. University-wide mandates impact the lives and well-being of not only Columbia members but other universities who take cues from the Ivy League, and they should not be made by a few specialists with little interdisciplinary expertise, viewpoint diversity and capacity to think critically and independently from bureaucracies with extensive financial conflicts of interest, and without soliciting input and debate with the wider University community.
3.Any University employee who was “suspended without pay” for refusing COVID vaccination, or whose medical or religious exemption request was denied, should be fully compensated for their lost wages. These coercive tactics are not ethical [10, 14], and especially for an experimental therapeutic whose effectiveness and safety risks are being obfuscated or whitewashed by those profiting from the product.
4.Any University member who took the vaccine because of the mandate, and who was injured or suffered systemic and long-lasting side effects from the vaccine that negatively affected their ability to work and function, should be offered a fair and generous opportunity to apply for compensation.
A well-publicized strategy and procedure for identifying and assisting such individuals should be implemented. Commit resources to promote research and development of interventions for vaccine injury.
5.Provide any and all documents related to how and why the University COVID policy making body decided to mandate COVID (as well as influenza) vaccination including key decisionmaker’s full financial disclosures and any ties with industry or other funding sources that could be perceived as a financial conflict of interest regarding the mandate.
It is critically important that university leadership give full and fair consideration and attention to all available evidence regarding vaccine risks and benefits because the current policies may be exposing University members to unnecessary medical risks and without true informed consent based on reliable global data.
In my view, university mandates clearly violate international human rights and informed consent standards as set forth by the Universal Declaration on Bioethics and Human Rights adopted unanimously by 193 countries including the US in 2005.13
Mounting evidence suggests that mRNA vaccines, particularly the PEG and spike glycoprotein components of all currently available COVID vaccines, are linked to increased risk for innate immune suppression and autoimmune, thrombotic, and cardiovascular side effects [5,9,11–14].
This letter serves to notify the university of potential liability for proceeding on the unfounded assumption that vaccines and boosters are sufficiently safe and effective in implementing its COVID-19 vaccine policies, especially for University students who are mostly 24 years old or younger. These misguided policies could potentially put the University’s endowment at risk.
At Columbia University, I have emailed and offered to meet with University leadership and decision makers several times since late summer 2021, and most recently in early June 2022, to present the current state of knowledge on vaccine safety research. I received one response in December 2021 from the University COVID response director.
Please see the references in this letter so the University can verify whether or not the University should blindly rely on recommendations from conflicted public health agencies. This letter also serves to notify the university that it may not be enough to rely on public health authorities to protect the university when global data clearly contradict the recommendations upon which the University’s policy relies.
We hope this letter will ultimately help to restore sanity and trust in the University’s public health policies and responses.
Please do not hesitate to let us know if we can be of service in guiding your University’s COVID vaccination policies in the future. Given the imminent deadlines for students to submit their exemption requests for Fall 2022, please respond to this letter via email (CC kevin@mermigislaw.com) by ___________.
We provide a preliminary list of co-signers below and links to the online version of the Columbia University letter which will be updated to include additional references as well as additional signatures which may be collected in August and this fall.
Sincerely,
Spiro P. Pantazatos, Ph.D.
Assistant Professor of Clinical Neurobiology at Columbia University Irving Medical Center
CU co-signers
Brian E. Scully, MD
Professor of Medicine at Columbia University Irving Medical Center (CUIMC) (Division of Infectious Diseases) and co-chair of Joint Infection Control Committee and Joint Antimicrobial Subcommittee of the Pharmacy Committee
Eric Urban, Ph.D. Professor of Mathematics and Director of Graduate Studies
Department of Mathematics at Columbia University
Claire-Marie Vacher, Ph.D.
Assistant Professor at CUIMC (Department of Pediatrics)
NewYork-Presbyterian Morgan Stanley Children’s Hospital
Non-CU co-signers
Kevin M. Barry, Esq.
Mermigis Law Group
85 Cold Spring Rd.
Syosset, NY 11791
kevin@mermigislaw.com
Libertynow.world, Co-Founder
Ioannis Papazoglou, Ph.D.
Shaun R. Barcavage, FNP-BC
Research Nurse Practitioner at Weill Cornell Medicine
Research Director at React19 (react19.org)
About the Author
To find more of Tessa Lena’s work, be sure to check out her bio, Tessa Fights Robots
- 1 PerspectivesOnThePandemic, Episode 25
- 2 FDA, November 30, 2020
- 3 Complaint for Declaratory and Injunctive Relief
- 4 Reuters, November 19, 2021
- 5 5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports Of Pf-07302048 (Bnt162b2) Received Through 28-Feb-2021, Table 2 and 7
- 6 PostMarketing Experience, Warnings and Precautions
- 7 Center for disease Control and Prevention, Myocarditis
- 8 Center for disease Control and Prevention, Adverse Events
- 9 Center for disease Control and Prevention, June 23, 2022 PDF
- 10 Jackanapes Junction Substack Jun 17, 2022
- 11 MSN January 11, 2022
- 12 Columbia News, September 01, 2021
- 13 Universal Declaration on Bioethics and Human Rights, 19 October 2005





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr