Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- Cardiologist, internist and epidemiologist Dr. Peter McCullough discusses why a key aspect of care — early treatment — has been missing from the pandemic
- With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection
- COVID-19 injections are waning in effectiveness and linked to an unacceptable number of serious injuries and deaths
- McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse; indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections
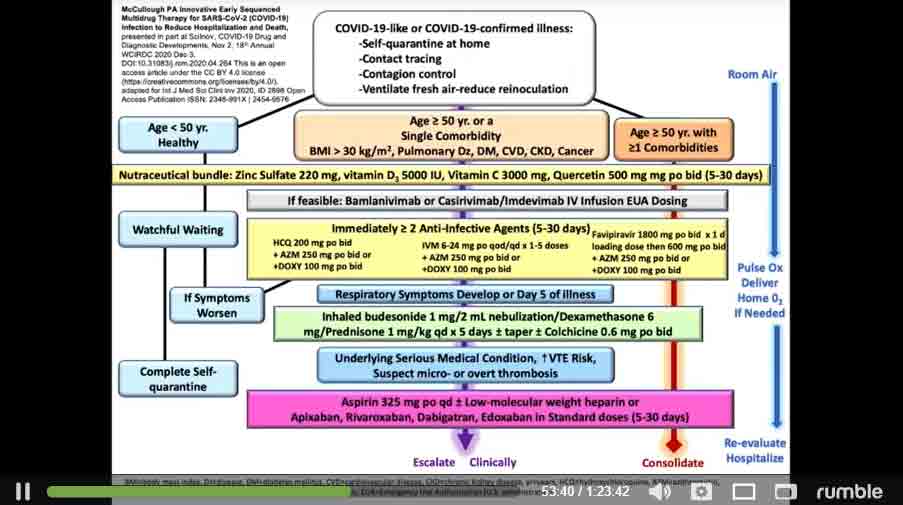
- At 53:40 in the video, you can view McCullough’s early treatment regimen, which initially includes a nutraceutical bundle, progressing to monoclonal antibody therapy, anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners
The video above,1 featuring cardiologist, internist and epidemiologist Dr. Peter McCullough, is packed with sound logic, data and action steps that have the potential to turn the pandemic around — if only more people would listen.
Recorded at the Andrews University Village Church in Berrien Springs, Michigan, August 20, 2021, this presentation deserves to be heard, and I urge you to listen to it in its entirety. It will make you question why a key aspect of care — early treatment — has been missing from the pandemic.
McCullough, editor of two medical journals who has published 650 peer-reviewed papers, said this has been the first time in his career when he saw medical providers not offering early treatment for a disease.
Early COVID Treatment Saves Lives
The standard of care for COVID-19 has been to withhold treatment until a person is sick enough to be hospitalized. It typically takes two to three weeks for someone with COVID-19 to get sick enough to be hospitalized, and during that time early treatment can be lifesaving.
The rationale was that there have been no large, randomized trials conducted to know which treatments are safe and effective, but as McCullough said, “We can’t wait for large randomized trials … Something got in the minds of doctors and nurses and everyone to not treat COVID-19. I couldn’t stand it.” He and colleagues worked feverishly to figure out a treatment — why didn’t national health organizations do so also?
“Our government and other governments, and the entire world, has not lifted a finger to reduce the risk of hospitalization and death anywhere,” McCullough said, pointing out the irony: “If there was a kid with asthma, would we let the kid wheeze and choke for two weeks before the kid has to go to the hospital? No, we give the child medications. We don’t have randomized trials for every single thing that we do.”2
McCullough and colleagues realized that there are three major phases to COVID-19. It starts with virus replication, which then triggers inflammation, or a cytokine storm. This, in turn, leads to blood clotting. If enough micro blood clots form in the lungs, a person can’t get enough oxygen and dies. It’s a complex process, and no single drug is going to work to treat it, which is why McCullough uses a combination of drugs, as is done to treat HIV, staph and other infections.
Only about 6% of doctors’ decisions in cardiology are based on randomized trials. “Medicine is an art and a science, it takes judgment. What was happening is, I think out of global fear, no judgement was happening,” McCullough said,3 referring to doctors’ refusal to treat COVID-19 patients early on in the disease process.
Doctors Threatened for Treating COVID-19
Around the world, the unthinkable is happening: Doctors are being threatened with loss of their license or even prison for trying to help their patients. French doctor Didier Raoult suggested, early on, putting up a tent to try to treat covid-19 patients. He was put on house arrest. He has promoted the use of hydroxychloroquine (HCQ), which initially was available over the counter — until France made it prescription only.4
In Australia, if a doctor attempts to treat a COVID-19 patient with HCQ, they could be put in prison. “Since when does a doctor get put in prison to try to help a patient with a simple generic drug?” McCullough said. In South Africa, he added, a doctor was put in prison for prescribing ivermectin.
In August 2020, McCullough’s landmark paper “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection” was published online in the American Journal of Medicine.5
The follow-up paper is titled “Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)” and was published in Reviews in Cardiovascular Medicine in December 2020.6 It became the basis for the home treatment guide.
While some physician organizations have stepped up and are treating COVID-19 patients, “The ivory tower today still is not treating patients. The party line in my health system is, do not treat a COVID-19 patient as an outpatient. Wait for them to get sick enough to be admitted. Because my health system … follows the National Institutes of Health or the Centers for Disease Control, period.”
Conditioned to Wait for an Injection
With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection. “We became conditioned, after about May or so, to wear a mask, wait in isolation and be saved by the vaccine. And wait for the vaccine. And all we could hear about is the vaccine.”
The injections were developed, but they’re different than any prior vaccines and have been losing effectiveness while causing an unacceptable number of serious injuries and deaths. For comparison, in 1976, a fast-tracked injection program against swine flu was halted after an estimated 25 to 32 deaths.7
According to McCullough in the video, if a new drug comes on the market and five deaths occur, the standard is to issue a black box warning stating the medication may cause death. With 50 deaths, the product is pulled from the market, he says. Now consider this: The Vaccine Adverse Event Reporting System (VAERS) database showed that — for all vaccines combined before 2020 — there were about 158 total deaths reported per year.
By January 22, 2021, there were already 182 deaths reported for COVID-19 injections, with just 27.1 million people vaccinated. This was more than enough to reach the mortality signal of concern to stop the program, McCullough said.
“We’ve already crossed the line of concern January 22. And if there was a data safety monitoring board — I know, because I do this work — we would have had an emergency meeting and said, wait a minute, people are dying after the vaccine. We’ve got to figure out why.”8
It’s standard to have an external critical event committee, an external data safety monitoring board and a human ethics committee for large clinical trials — such as the mass COVID-19 injection program, but these were not put into place.
“This is something we’ve never seen in human medicine — a new product introduced and just going full-steam ahead with no check on why people are dying after the vaccine,” McCullough said. On two occasions, the CDC and FDA — in March and in June — reviewed the data and said none of the deaths are related to the vaccines. “I think this is malfeasance,” he stated.
Fast-forward to July 30, 2021, and VAERS data showed 12,366 Americans have died after a COVID0-19 injection.9 In an analysis of COVID-19 vaccine death reports from VAERS, researchers found that 86% of the time, nothing else could have caused the death, and it appears the vaccine was the cause.10
The Spike Protein Is Dangerous
Your body recognizes the spike protein in COVID-19 jabs as foreign, so it begins to manufacture antibodies to protect you against COVID-19, or so the theory goes. But there’s a problem. The spike protein itself is dangerous and known to circulate in your body at least for weeks and more likely months11 — perhaps much longer — after the COVID jab.
In your cells, the spike protein damages blood vessels and can lead to the development of blood clots.12 It can go into your brain, adrenal glands, ovaries, heart, skeletal muscles and nerves, causing inflammation, scarring and damage in organs over time. McCullough also believes that the spike protein is present in donated blood, and they’ve notified the Red Cross and the American Association of Blood Banking.
Messenger RNA (mRNA) platforms have been under study for years, in most cases being designed to replace a defective gene, which could potentially be used for cancer or heart failure treatment, for example.
In November 2020, however, Pfizer, in a joint venture with Germany-based BioNTech, announced that their mRNA-based injection was “more than 90% effective” in a Phase 3 trial.13 This does not mean that 90% of people who get injected will be protected from COVID-19, as it’s based on relative risk reduction (RRR).
The absolute risk reduction (ARR) for the jab is less than 1%. “Although the RRR considers only participants who could benefit from the jab, the absolute risk reduction (ARR), which is the difference between attack rates with and without a jab, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs,” researchers wrote in The Lancet Microbe in April 2021.14
McCullough believes the mass injection campaign is an incredible violation of human ethics, in part because no one should be pressured, coerced or threatened into using an investigational product.
No attempts have been made to present or mitigate risks to the public, such as giving it only to people who really need it — not to low risk groups like children and young people and those who are naturally immune to COVID-19 due to prior infection. “I think this is the most disturbing thing,” he said.
The Injections Don’t Stop COVID-19, Can Be Deadly
The CDC’s Morbidity and Mortality Weekly Report (MMWR) posted online July 30, 2021, details an outbreak of COVID-19 that occurred in Barnstable County, Massachusetts — 74% of the cases occurred in fully vaccinated people.15
Indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections. Their effectiveness, too, is rapidly waning. A study published in medRxiv, using data from the Mayo Clinic Health System, revealed that during periods of Alpha and Delta variant prevalence, Moderna’s injection was 76% effective while Pfizer’s effectiveness was only 42%.16
A little-known fact is that Moderna’s jab has three times the dose of Pfizer’s, but, curiously, health officials aren’t even discussing this or giving the public updates on which of the three injections work “best.” The narrative is simple and straightforward — get an injection, any injection.
Yet, as McCullough noted, the virus has mutated, and the vaccines aren’t working the way health officials had hoped: “The vaccines don’t stop COVID-19, at least not completely, and they’re not a shield against mortality.”17
Similar to VAERS, the U.K. maintains a “Yellow Card” reporting site to report adverse effects to vaccines and medications.18
Tess Lawrie, whose company The Evidence-Based Medicine Consultancy has worked with the World Health Organization, analyzed U.K. Yellow Card data and concluded that there’s more than enough evidence to pull the injections from the market because they’re not safe for human use. The report stated:19
“It is now apparent that these products in the blood stream are toxic to humans. An immediate halt to the vaccination programme is required whilst a full and independent safety analysis is undertaken to investigate the full extent of the harms, which the UK Yellow Card data suggest include thromboembolism, multisystem inflammatory disease, immune suppression, autoimmunity and anaphylaxis, as well as Antibody Dependent Enhancement (ADE).”
Early Treatment Is Crucial
McCullough is trying to get the word out about the importance of early treatment of COVID-19. Early ambulatory therapy with a sequenced-multidrug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile to reduce the risk of hospitalization and death.
At 53:40 in the video, you can view McCullough’s early treatment regimen, which initially includes a nutraceutical bundle. While you’re recovering at home, open your windows and get plenty of fresh air and ventilation in your home.
If symptoms persist or worsen, he recommends calling your doctor and demanding monoclonal antibody therapy. The treatment progresses to include anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners.
If your doctor refuses to treat COVID-19 in the early stages, find a new one and/or visit a telemedicine clinic that will help, as “the prehospital phase is the time of therapeutic opportunity.”
McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse. They “have an unfavorable safety profile and are not clinically effective, thus they cannot be generally supported in clinical practice at this time.”
Logically, this is clear, but McCullough believes we’re dealing with a mass psychosis that is preventing people from seeing the light. “The whole world is in a trance,” he said, adding:20
“Things are getting disturbingly out of control and it’s in the context of the virus. It is clear … we are in a very special time in the history of mankind. Whatever is going on, it is the entire world … every human being in the world. It appears to have a program.
The program … is happening to promote as much fear, isolation, suffering, hospitalization and death in order to get a needle in every arm, at all costs. That is what’s going on, and no one in this room can disagree.”
- 1, 2, 3, 4, 8, 9, 17, 20 Rumble August 26, 2021
- 5 American Journal of Medicine January 2021; 134(1): 16-22
- 6 Reviews in Cardiovascular Medicine 2020; 21(4): 517-530
- 7 CNN April 30, 2009
- 10 ResearchGate Preprint June 2021
- 11 Clinical Infectious Diseases, ciab465, doi: 10.1093/cid/ciab465
- 12 Bitchute July 22, 2021
- 13 Pfizer November 9, 2020
- 14 The Lancet Microbe April 20, 2021
- 15 MMWR Weekly August 6, 2021 / 70(31);1059-1062
- 16 medRxiv. 2021 Aug 9;2021.08.06.21261707. doi: 10.1101/2021.08.06.21261707
- 18 Yellow Card
- 19 The Evidence-Based Medicine Consultancy June 9, 2021





")












Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr