Analysis by Dr. Joseph Mercola
STORY AT-A-GLANCE
- A recent report details a SARS-CoV-2 Delta outbreak in an Israeli hospital where 238 out of 248 (96%) of the exposed patients and staff had been fully vaccinated with Pfizer’s mRNA vaccine
- Of the 238 fully vaccinated individuals, 39 (16%) were infected, as were three of the 10 unvaccinated individuals who got exposed
- While all of the sickened staff recovered, five infected patients died and nine turned into severe or critical cases. All of the dead and severe/critical cases were fully vaccinated. Two unvaccinated patients that got infected only had mild illness
- This outbreak tells us that the COVID shots cannot create herd immunity. It also suggests vaccinated people may be more prone to serious and lethal infection than the unvaccinated
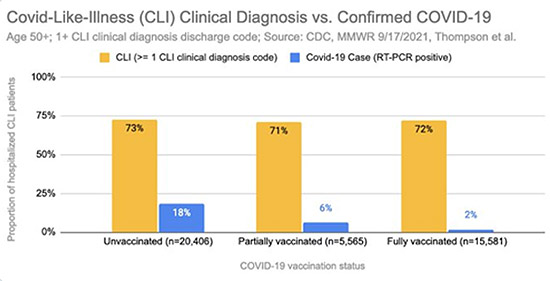
- Of 41,552 hospitalized patients in the U.S., 73% of the unvaccinated, 71% of the partially vaccinated and 72% of the fully vaccinated received a diagnosis of COVID-like illness (CLI) between January 1, 2021, and June 22, 2021
As we enter into the 10th month of COVID injections, what can we tell about their effectiveness? Are they working? According to data from Israel — which is the best in the world at this point, thanks to the Israelis’ dedication to data collection and transparency — it seems the news is anything but good, and that is a profoundly serious understatement.
In an October 3, 2021, substack article,1 Alex Berenson dissects a recent Eurosurveillance report2 about a SARS-CoV-2 Delta outbreak in an Israeli dialysis ward. Eurosurveillance is a journal published by the European Centers for Disease Control.
Hospital Outbreak Reveals the Ineffectiveness of COVID Jabs
An unidentified dialysis patient came in for scheduled treatment with fever and cough. Over the course of several days, his condition continued to deteriorate, but he remained in the dialysis unit at the Meir Medical Center.
COVID measures at the hospital includes routine wearing of full protective equipment by all COVID unit staff, including N-95 mask, face shield, gown, gloves and hair cover. Patients also wear surgical masks when in the same room as another patient.
By the time the sick patient was tested and diagnosed with COVID-19, he had a PCR cycle threshold (CT) of 13.6, which means he had a viral load approximately 1 million times higher than a person with mild infection.
The infection spread rapidly among patients and staff, spreading from the dialysis ward to the COVID-19 ward and other units. At the time of the outbreak, 238 out of 248 (96%) of the exposed patients and staff had been fully vaccinated with Pfizer’s mRNA vaccine. Of the 238 fully vaccinated individuals, 39 (16%) were infected, as were three of the 10 unvaccinated individuals who got exposed.
Near-Maximum Vaccination Rate Yet No Herd Immunity
While all of the sickened staff recovered, five infected patients died and nine turned into severe or critical cases. All of the dead and severe/critical cases were fully vaccinated. Two unvaccinated patients who were infected only had mild illness. As noted by the authors:3
“The calculated attack rate among all exposed patients and staff was 10.6% (16/151) for staff and 23.7% (23/97) for patients, in a population with 96.2% vaccination rate (238 vaccinated/248 exposed individuals).
Moreover, several transmissions probably occurred between two individuals both wearing surgical masks, and in one instance using full PPE, including N-95 mask, face shield, gown and gloves …
This nosocomial outbreak exemplifies the high transmissibility of the SARS-CoV-2 Delta variant among twice vaccinated and masked individuals. This suggests some waning of immunity, albeit still providing protection for individuals without comorbidities …
This communication … challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks…
In the outbreak described here, 96.2% of the exposed population was vaccinated. Infection advanced rapidly (many cases became symptomatic within 2 days of exposure), and viral load was high.
Another accepted view is that, when facing a possible mismatch between the SARS-CoV-2 variant and vaccine or waning immunity, the combination of vaccine and face mask should provide the necessary protection.
Although some transmission between staff members could have occurred without masks, all transmissions between patients and staff occurred between masked and vaccinated individuals, as experienced in an outbreak from Finland.”
This case tells us a couple of important things. First, that even in a population where more than 96% are fully vaccinated, outbreaks will occur. This means the shots are clearly not even remotely creating any kind of herd immunity. Indeed, there have been outbreaks even in populations where the vaccination rate was 100%.4
Secondly, the unvaccinated who got sick had only mild illness, while the fully vaccinated all ended up with severe infection. The unvaccinated recovered without a problem while several of the fully vaccinated patients died.
Thirdly, it tells us masks, face shields and gloves provide little more than a false sense of security. Altogether, this report is evidence that everything we’re currently doing is foolishness.
COVID-Like Illness Among the Vaccinated
In the U.S., the data are far more manipulated, as this next section will reveal. The study5 in question, “Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings,” was published September 8, 2021, in The New England Journal of Medicine.
The researchers identified a total of 103,199 hospitalizations between January 1, 2021, and June 22, 2021. Of those, 41,552 met the study criteria for inclusion (the real number is actually 41,159, as there’s a mathematical error6). Included patients were 50 or older, and had “COVID-like illness” (CLI), defined as COVID symptoms and a positive PCR test.
Excluded hospitalizations that did not meet the study criteria were patients younger than 50, patients without vaccination record, repeat admissions, patients that had no COVID test results, and those who had received their second dose of mRNA injection (or first and only dose required of the Janssen vaccine) within the last 14 days and therefore were not considered fully vaccinated.
The exclusion of people who got the jab within 14 days of their hospitalization is more than regrettable and designed to create real misinformation and fraudulent results skewed in favor of the jab. Researchers have determined that you’re at increased risk of infection during the first 14 days, because you haven’t reached adequate antibody levels yet.
A Swedish study7 posted April 21, 2021, found “The estimated vaccine effectiveness in preventing infection ?7 days after second dose was 86% but only 42% ?14 days after a single dose.” While maximum effectiveness isn’t reached until the 14-day mark, why shouldn’t hospitalizations that occur within that two-week window count?
According to The New England Journal of Medicine report, the effectiveness of the mRNA shots against lab-confirmed SARS-CoV-2 infection, 14 or more days after injection, was 89%, on average. Effectiveness among those 85 and older, those with chronic medical conditions, as well as Black and Hispanic adults, ranged from 81% to 95%.
The effectiveness of the Janssen “vaccine” against lab-confirmed infection leading to hospitalization was 68%, and 73% against infection requiring emergency care. That sounds pretty good, but it doesn’t tell the whole story.
Digging Further Into the Data
In a Twitter thread,8 Ben M. double-checked and recalculated the vaccine efficacy, taking into account all CLI admissions, not just those where the patient had been vaccinated at least 14 days prior. When adding those previously excluded patients back in, Ben M. came up with a vaccine effectiveness rate of 13%.
He also discovered that if you look at how many people actually had a CLI clinical diagnosis code among the 41,552 included patients, the rate of diagnosis between the unvaccinated, the partially vaccinated and the fully vaccinated was nearly identical: 73% for the unvaccinated, 71% for the partially vaccinated and 72% for the fully vaccinated.
Here’s where it gets interesting. When you look at the rate of CLI, and add in the rate of positive PCR tests, all of a sudden, differences between the groups become clear. Only 2% of the fully vaccinated had a positive PCR test, compared to 6% of the partially vaccinated and 18% of the unvaccinated.
Ben M. speculates that vaccinated patients may be tested less routinely (12.5% less frequently to be exact), or unvaccinated patients are tested more routinely (11% more frequently than the vaccinated). But there may be another explanation. The U.S. Centers for Disease Control and Prevention actually has two different sets of testing criteria, depending on the patient’s vaccination status.
Fully vaccinated individuals suspected of having contracted COVID-19 are to be tested using a CT of 28 or less, whereas unvaccinated patients are to be tested using a CT of 40.
Anything over 35 CTs has been shown to produce 97% false positives,9 so this biased testing guidance virtually guarantees that vaccinated patients are more likely to test negative, while unvaccinated patients are more likely to get a false positive.
Partially Vaxxed Are the Most Symptomatic for CLI
What’s more, when Ben M. looked at symptoms alone, he found that the partially vaccinated are the most symptomatic for CLI (29.2%), followed by the fully vaccinated (28.1%) and then the unvaccinated (27.4%).
When he then recalculated vaccine effectiveness based on symptomatic CLI alone (i.e., with or without a positive test), it again came out negative: -6% in the partially vaccinated and -3% in the fully vaccinated. As noted by Ben M. “this means that despite COVID-19 vaccination, people appear to get as sick and hospitalized (if not even more!), as before?!”
He provides a whole series of helpful visuals in his Twitter thread, so to get a clearer idea, I recommend reading through it and looking through all the graphs provided.10 In summary, what Ben M. discovered is that:
•The rate of CLI admission, diagnosis and symptoms are nearly identical between the unvaccinated and vaccinated, so there’s no indication that the COVID shot reduces CLI.
•Sample exclusions distort the data, making the COVID shots appear more effective.
•Of the included hospitalizations for CLI, 53% were either partially or fully vaccinated, compared to 47% unvaccinated.
As of June 15, 2021, 48.7% of Americans were fully “vaccinated,”11 so the distribution of unvaccinated and fully vaccinated individuals being admitted to hospital should have been close to 50/50 by June 22, 2021, which was the cutoff date in this study.
The rate of partially vaccinated has trended about 8% to 10% higher, which would put the vaccinated to unvaccinated ratio at around 60/40. If you assume the number of vaccinated people over the age of 50 was the same as the number of unvaccinated, or just slightly higher, the fact that 53% of CLI cases were vaccinated and 47% were unvaccinated, it suggests the rate of CLI is nearly identical regardless of vaccination status.
•To tease out why vaccinated people develop CLI at the same rate as the unvaccinated, we need all-cause hospitalization and death data by vaccination status, but even though the CDC has acknowledged to Ben M. that they have this data, they denied his Freedom of Information Act request to obtain it.
No Correlation Between Vaccination Rates and COVID Cases
In related news, Blaze Media recently reported the findings of Harvard researchers, who found “absolutely no correlation between vax rates and COVID cases globally.”12 The paper’s title tells you pretty much tells the whole story and everything you need to know: “Increases in COVID-19 Are Unrelated to Levels of Vaccination Across 68 Countries and 2,947 Counties in the United States.”13 According to the authors:
“… the narrative related to the ongoing surge of new cases in the United States (US) is argued to be driven by areas with low vaccination rates. A similar narrative also has been observed in countries …
We used COVID-19 data provided by the Our World in Data for cross-country analysis, available as of September 3, 2021 …We included 68 countries that met the following criteria: had second dose vaccine data available; had COVID-19 case data available; had population data available; and the last update of data was within 3 days prior to or on September 3, 2021.
For the 7 days preceding September 3, 2021 we computed the COVID-19 cases per 1 million people for each country as well as the percentage of population that is fully vaccinated … The percentage increase in COVID-19 cases was calculated based on the difference in cases from the last 7 days and the 7 days preceding them …
At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days. In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.
Notably, Israel with over 60% of their population fully vaccinated had the highest COVID-19 cases per 1 million people in the last 7 days. The lack of a meaningful association between percentage population fully vaccinated and new COVID-19 cases is further exemplified, for instance, by comparison of Iceland and Portugal.
Both countries have over 75% of their population fully vaccinated and have more COVID-19 cases per 1 million people than countries such as Vietnam and South Africa that have around 10% of their population fully vaccinated.
Across the U.S. counties too, the median new COVID-19 cases per 100,000 people in the last 7 days is largely similar across the categories of percent population fully vaccinated … There also appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated …
The sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences needs to be re-examined … Other pharmacological and non-pharmacological interventions may need to be put in place alongside increasing vaccination rates.
Such course correction, especially with regards to the policy narrative, becomes paramount with emerging scientific evidence on real world effectiveness of the vaccines.
For instance, in a report released from the Ministry of Health in Israel, the effectiveness of 2 doses of the BNT162b2 (Pfizer-BioNTech) vaccine against preventing COVID-19 infection was reported to be 39%, substantially lower than the trial efficacy of 96%.
It is also emerging that immunity derived from the Pfizer-BioNTech vaccine may not be as strong as immunity acquired through recovery from the COVID-19 virus. A substantial decline in immunity from mRNA vaccines 6-months post immunization has also been reported.
Even though vaccinations offers protection to individuals against severe hospitalization and death, the CDC reported an increase from 0.01 to 9% and 0 to 15.1% (between January to May 2021) in the rates of hospitalizations and deaths, respectively, amongst the fully vaccinated.”
- 1 Alex Berenson Substack October 3, 2021
- 2, 3 Eurosurveillance September 2021; 26(39)
- 4 FBA News August 9, 2021
- 5 The New England Journal of Medicine September 8, 2021 DOI: 10.1056/NEJMoa2110362
- 6, 8, 10 Twitter Ben M September 30, 2021
- 7 MedRxiv April 21, 2021 DOI: 10.1101/2021.04.20.21254636
- 9 Clinical Infectious Diseases September 28, 2020; ciaa1491
- 11 Mayo Clinic COVID Vaccine Tracker
- 12 Blaze Media October 5, 2021
- 13 European Journal of Epidemiology September 30, 2021





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr