STORY AT-A-GLANCE
- Jodi O’Malley, a registered nurse who works for the U.S. Department of Health and Human Services’ Indian Health Services branch in Phoenix, Arizona, is blowing the whistle on COVID jab injuries
- A DHHS emergency room physician admits no one is reporting COVID jab injuries, even though it’s required for emergency use medications
- According to media reports, unvaccinated COVID patients are causing health care systems to be overwhelmed. Health care systems in Idaho, Alaska and Montana have started rationing health care based on probability of survival
- What many media outlets are not addressing is that medical resources are under strain due to the enormous numbers of trained medical staff either resigning or getting fired for refusing the COVID jab
- Public health data are being massively manipulated and then wielded as a weapon to justify egregious power grabs and governmental overreaches. In the process, the medical profession has been pushed to the edge of a moral void where patients are viewed as disposable based on their medical choices
In Part 1 of the video above, Project Veritas interviews Jodi O’Malley, a registered nurse who works for the U.S. Department of Health and Human Services’ Indian Health Services branch in Phoenix, Arizona.
O’Malley is blowing the whistle with taped recordings in which HHS staff express concern and disgust over the fact that the federal government is hiding and not addressing COVID jab injuries, which are now flooding hospitals.
Dr. Maria Gonzales, a DHHS emergency room physician, is heard saying that vaccine injuries are not being reported as required for emergency use medications. She also suspects studies aren’t done because “the government doesn’t want to show that the … vaccine is full of shit.”
As noted by O’Malley, the public is participating in a Phase 3 drug trial, and that’s the stage when you would normally collect safety data. It’s the responsibility of everyone involved to make sure that data are collected and reported. Yet a majority of vaccine injuries are simply written off as unrelated.
Even when a link is suspected or blatantly obvious, it’s rarely reported because it’s a time-consuming process. So, “how are we going to say that this [“vaccine”] is safe and approved for use?” O’Malley asks. O’Malley lost a coworker to the COVID shot. The nurse didn’t want to get it due to religious objections, but was coerced into it. Shortly after her first shot, she was hospitalized and died.
‘Evil at the Highest Levels’
Ivermectin, meanwhile, which has virtually no side effects and has been shown to effectively treat COVID-19, is prohibited within the DHHS. When O’Malley asks Gayle Lundberg, a DHHS pharmacist, if ivermectin can be given to a patient if the doctor is willing to prescribe it, Lundberg responds:
“I am stuck. I am told you are absolutely not to use [ivermectin] under any circumstances whatsoever for somebody with COVID, unless you don’t want to have a job. I’m not going to lose my job over this.”
“This is evil at the highest level,” O’Malley says. “You have the FDA, the CDC, that are both supposed to be protecting us, but they are under the government, and everything we’ve done so far is unscientific.”
The Nursing Shortage Is a Dictatorship-Made Crisis
We’re now told there’s a massive nursing shortage, and that unvaccinated COVID patients are causing health care systems to be overwhelmed. September 16, 2021, The Associated Press reported health care systems in Idaho, Alaska and Montana have started rationing health care as medical resources are being exhausted from an influx of COVID-19 patients.1
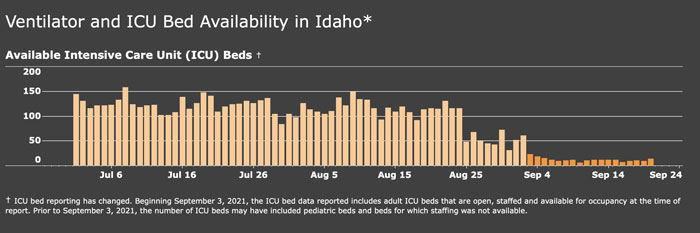
According to the HHS Protect Public Data Hub,2 Idaho’s hospitals were at 70.27% capacity as of September 23, 2021, and only 20.51% of inpatient beds were in use for COVID-19. Idaho’s intensive care units, on the other hand, were near capacity at 90.8%, with 62.34% of ICU beds being in use for COVID-19.
These numbers change by the day but, not surprisingly, the influx is blamed on people refusing to get the COVID shot. Idaho Department of Health and Welfare leadership reportedly told hospitals to implement “crisis standards of care,”3 meaning allotting ICU beds to patients “most likely to survive,” while treating other patients with “less effective methods” or palliative care only.
A hospital in Helena, Montana, has also implemented crisis standards of care, as has the Providence Alaska Medical Center.
However, what many media outlets are not addressing is the fact that medical resources are under strain due to the enormous numbers of trained medical staff either resigning or getting fired for refusing the jabs.
As reported by FEE.org, Houston hospitals “have reached a breaking point” due to the loss of several hundred hospital workers. Houston Methodist Hospital fired 150 of its staff, the Harris Health System is short 250 workers and the University of Texas Medical Branch is short 100:4
“’All last year, through the COVID pandemic, we came to work and did our jobs,’ said Kara Shepherd, a labor and delivery nurse … ‘We did what we were asked. This year, we’re basically told we’re disposable’ …
When hospital administrators set their policy — get vaccinated or lose your job — their goal was to increase vaccination rates of hospital staff. The unintended consequence was a shortage of nurses and other hospital workers during a deadly pandemic.”
Texas Gov. Greg Abbott has reportedly requested 2,500 out of state nurses to help with the statewide crisis.5 Whether he’ll be able to get them is another question, seeing how states that have issued the same vaccine mandates are dealing with the same shortage problems. Critical nursing shortages are reported in South Carolina6 and Maryland,7 for example, two states where hospitals have implemented COVID jab mandates.
COVID Hospitalizations or Media Hallucinations?
Of course, with all the fake narratives floating around, it’s hard to tell whether the COVID crisis is actually real. Are hospitals struggling simply because they ditched too many of their staff? Are hospitalized patients there for reasons other than COVID and simply happen to test positive using faulty PCR testing?
Are vaccine injuries being mislabeled as unvaccinated COVID cases simply because they’re hospitalized before they’re officially “fully vaccinated”? Are we seeing an influx of sick patients due to vaccine-induced antibody dependent enhancement, which makes you more susceptible to infection?
It’s virtually impossible to tell what’s what, as the data is being intentionally obfuscated. For example, you’re not counted as fully vaccinated until 14 days after your second dose,8 so if you’re hospitalized before then, you’re logged as “unvaccinated.” The U.S. Centers for Disease Control and Prevention also has two different sets of testing criteria, depending on the patient’s vaccination status.
Fully vaccinated individuals suspected of having contracted COVID-19 are to be tested using a cycle threshold (CT) of 28 or less, whereas unvaccinated patients are to be tested using a CT of 40. Anything over 35 CTs has been shown to produce 97% false positives,9 so this biased testing guidance is blatant in what it’s trying to achieve.
The American Medical Association is also instructing doctors to redefine COVID hospitalizations as “deaths” when communicating with media or the public,10 and according to whistleblowers, what the media and hospital administrators are calling Delta cases are really vaccine injuries.11
According to a recent study12,13 of hospitalization records, between March 2020 and early January 2021, 36% of COVID hospitalizations were for mild or asymptomatic disease. Between mid-January 2021 and the end of June 2021, that number rose to 48%. So, nearly half of all COVID hospitalizations may in reality be for other health problems (the patient simply tested positive when admitted for something else), or for mild infection.
With regard to Idaho, the state changed the way they count available ICU beds September 3, 2021, which caused the number of available ICU beds to dramatically drop.14
Sadly, this is far from a complete list of all the ways in which data are being manipulated and twisted. But, as you can imagine, even one of these strategies is enough to muddle the waters. Add them all together and what you have is a situation in which there’s no possible way to get a clear picture of what’s really going on.
Public Health as an Objective Reality Must Be Rejected
What we do know is that public health data are now being wielded as a weapon to justify any number of egregious power grabs and governmental overreaches. Hence all the manipulation of said data.
With each passing day, it’s becoming clearer that a biosecurity state is being erected around us. People are being stripped of their health, their lives and their livelihoods in the name of public health. As noted by Christopher Lingle in his American Institute for Economic Research July 29, 2021, article:15
“… fear ginned up during the recent pandemic based on pronouncements reflecting ‘expert’ authority caused individuals to stop thinking of health as a personal issue and to embrace ‘public health.’ The notion that ‘public health’ reflects an objective reality must be challenged, especially since so much focus is on only one among many viruses and on only one disease among many ailments that afflict mankind.
It is troubling that these political feats of legerdemain have induced many citizens to accept an artificial collective construct, with solidarity dominating individual autonomy and security elevated over human liberty …
Should citizens resist limits on their individual liberty and rights to achieve collective goals, authoritarian repression becomes an inevitable instrument to ‘pacify’ the masses.
Such excesses and abuse of State power occurred over a vast range of collectivist regimes. For example… [o]ne element of the philosophy of the Nazi Party … promoted the good of the whole over the good of the individual …
Medical technicians, central to the operations of the Nazi State, perpetuated scientific nostrums of evolution and genetic hygiene based on eugenics to advance racial purity. Many Nazi supporters in the early days of the regime may never have imagined the terrible outcomes of following this foul ideology.
As such, caution should be applied to assess the ‘scientific’ wisdom that informs anxieties over deterioration of the natural environment or the health of members of a community. Just as many of the accepted truths of the Green movement are based upon selective application of science, so are the ‘truths’ guiding health policies in the time of Covid-19.”
The Importance of Moral Philosophy
Speaking of Nazis, just how and why did so many medical professionals join the Nazi party and choose to participate in the genocide? In a December 2020 article in Tablet magazine,16 bioethicist Dr. Ashley Fernandes took a deep dive into these questions.
She points out that the one discipline that connects medicine and law is moral philosophy. “Both law and medicine involve reason and the will, directed toward the good of the person,” she writes. The Holocaust occurred because moral philosophy was corrupted first. The practice of medicine then followed in the same tracks.
Tragically, we’re seeing the same thing happen now, right before our eyes. Early on in the pandemic, a nurse stationed at Elmhurst Hospital at the epicenter of the pandemic in New York City blew the whistle saying patients were being killed for profit and wrote a book about it.17 As soon as hospitals were given large payments for COVID patients, every patient became a COVID-19 patient.
At Elmhurst Hospital, patients were labeled as COVID-19 even if they had a negative test and no symptoms. Most were placed on mechanical ventilation, which killed them. Similar stories emerged from other countries as well.
To this day, around the U.S., doctors, nurses and pharmacists who ought to know better are simply following orders handed down from above. The pharmacist’s sentiment that “I’m not losing my job over this,” is probably a common one. Meanwhile, COVID patients are treated to death with provably ill-advised protocols.
As if that weren’t enough, we’re now seeing hospitals rationing care, and a number of doctors and health officials have said the unthinkable out loud, which is that they want to block unvaccinated people from getting any medical care whatsoever.18,19 Australia is going down that path already. In other words, some think you don’t have a right to life if you decide not to play medical Russian roulette and get the COVID jab.
This is the result of allowing a decay of ethics and morals to gain foothold, and the only people who can stop this spreading rot is us. Like O’Malley, each and every one of us must decide what kind of person we want to be. There may be a price to pay for refusing to contribute to the gangrenous machinations underway, but there will be a price to pay if we don’t as well, and it’s likely to be far more painful in the end.
“Even granting the (disputable) claim that the primary motivation for the Holocaust was economic or political, the Nazis somehow made the leap from identifying persons as ‘economic drains’ to becoming completely and utterly disposable,” Fernandes writes.20
“Physicians, dressed in white coats, gave the imprimatur that indeed, those that were to be gassed were not human persons at all … Robert N. Proctor (1988) notes that physicians joined the Nazi party in droves (nearly 50% by 1945), much higher than any other profession.
Physicians were seven times more likely to join the SS than other employed German males. Nurses were also major collaborators. The Holocaust should be studied by every health care professional as a reminder of how sacred the substance of our craft is, and what the consequences may be if we forget the dignity of persons again.”
Five Lessons to Prevent Another Genocide
Fernandes goes on to list five lessons of Nazi medicine that must be remembered and integrated into medical practice “if medicine is to survive as a profession of healing” and not serve as a tool for genocide again:21
1.Health professionals and society at large must affirm a strong personalism — Personalism posits that “the ultimate unit of value of human life is the individual person herself.” Society is created for the individual, not the other way around. Hence the dignity and integrity of each individual person must be held sacrosanct.
2.We must have “rigorous conscience protection for physicians and health care providers” — Contemporary bioethics favor removal of conscience protection laws and forcing doctors to perform procedures they find amoral.
Abortion, contraception, circumcision, sterilization and euthanasia are but a few examples. Forcing health professionals to act against their own conscience breeds the kind of moral rot we’re now faced with as medical staff act against their better judgment.
3.Affirm that science is not a “god” — Science relies on hypotheses, experimentation and testing of those hypotheses. But it cannot answer whether a medical practice is ethical and morally good. For that, we need moral philosophy, which is rooted in reason and lived experience. “The ethical enterprise is therefore both objective (rational) and subjective (experiential),” Fernandes writes.
4.Health professionals must resist the desensitization to dehumanization, which includes using derogatory terms to describe patients — As noted by Fernandes, “it is far easier to kill a ‘vegetable’ than a human person … Language alters perception, and perception affects our ethical calculus.”
5.As a physician, you must vow to exclusively serve the patient, “not some abstracted idea of ‘society’” — Fernandes adds, “Today we seem to be losing more of our commitment to the individual patient — for there are other ‘gods’ in medicine.
‘Quality of life,’ ‘public health’ or even ‘patient satisfaction’ have become ends in themselves, not a means to an end … [The] power of the ‘white coat’ demands, if we are to fulfill our obligations of trust, that we do not serve the state (and its economic interests), nor the patient’s family … nor any other ‘just cause’ or goal, including our own.”
- 1, 3 AP September 16, 2021
- 2 HHS Protect Public Data Hub, Idaho selected from dropdown menu, data as of 9/22/21
- 4, 5 FEE August 18, 2021
- 6 Wyff4 September 21, 2021
- 7 WBALTV September 22, 2021
- 8 CDC September 16, 2021
- 9 Clinical Infectious Diseases September 28, 2020; ciaa1491
- 10 AMA COVID-19 Guide
- 11 Red Voice Media September 8, 2021
- 12 Research Square September 13, 2021
- 13 The Atlantic September 13, 2021
- 14 Twitter Tessa Fights Robots September 20, 2021
- 15 American Institute for Economic Research July 31, 2021
- 16, 20, 21 Tablet December 10, 2021
- 17 Amazon
- 18 USA Today September 5, 2021
- 19 THV11 August 17, 2021





")











Thanks! Share it with your friends!
Tweet
Share
Pin It
LinkedIn
Google+
Reddit
Tumblr